Community-acquired infections Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(1):71-78
DOI 10.5935/0103-507X.20190013
To compare the clinical characteristics and outcomes of patients with community-acquired and hospital-acquired sepsis.
This is a retrospective cohort study that included all patients with a diagnosis of sepsis detected between January 2010 and December 2015 at a private hospital in southern Brazil. Outcomes (mortality, intensive care unit and hospital lengths of stay) were measured by analyzing electronic records.
There were 543 hospitalized patients with a diagnosis of sepsis, with a frequency of 90.5 (85 to 105) cases/year. Of these, 319 (58%) cases were classified as hospital-acquired sepsis. This group exhibited more severe disease and had a larger number of organ dysfunctions, with higher hospital [8 (8 - 10) versus 23 (20 - 27) days; p < 0.001] and intensive care unit [5 (4 - 7) versus 8.5 (7 - 10); p < 0.001] lengths of stay and higher in-hospital mortality (30.7% versus 15.6%; p < 0.001) than those with community-acquired sepsis. After adjusting for age, APACHE II scores, and hemodynamic and respiratory dysfunction, hospital-acquired sepsis remained associated with increased mortality (OR 1.96; 95%CI 1.15 - 3.32, p = 0.013).
The present results contribute to the definition of the epidemiological profile of sepsis in the sample studied, in which hospital-acquired sepsis was more severe and was associated with higher mortality.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):71-78
DOI 10.5935/0103-507X.20190013
To compare the clinical characteristics and outcomes of patients with community-acquired and hospital-acquired sepsis.
This is a retrospective cohort study that included all patients with a diagnosis of sepsis detected between January 2010 and December 2015 at a private hospital in southern Brazil. Outcomes (mortality, intensive care unit and hospital lengths of stay) were measured by analyzing electronic records.
There were 543 hospitalized patients with a diagnosis of sepsis, with a frequency of 90.5 (85 to 105) cases/year. Of these, 319 (58%) cases were classified as hospital-acquired sepsis. This group exhibited more severe disease and had a larger number of organ dysfunctions, with higher hospital [8 (8 - 10) versus 23 (20 - 27) days; p < 0.001] and intensive care unit [5 (4 - 7) versus 8.5 (7 - 10); p < 0.001] lengths of stay and higher in-hospital mortality (30.7% versus 15.6%; p < 0.001) than those with community-acquired sepsis. After adjusting for age, APACHE II scores, and hemodynamic and respiratory dysfunction, hospital-acquired sepsis remained associated with increased mortality (OR 1.96; 95%CI 1.15 - 3.32, p = 0.013).
The present results contribute to the definition of the epidemiological profile of sepsis in the sample studied, in which hospital-acquired sepsis was more severe and was associated with higher mortality.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
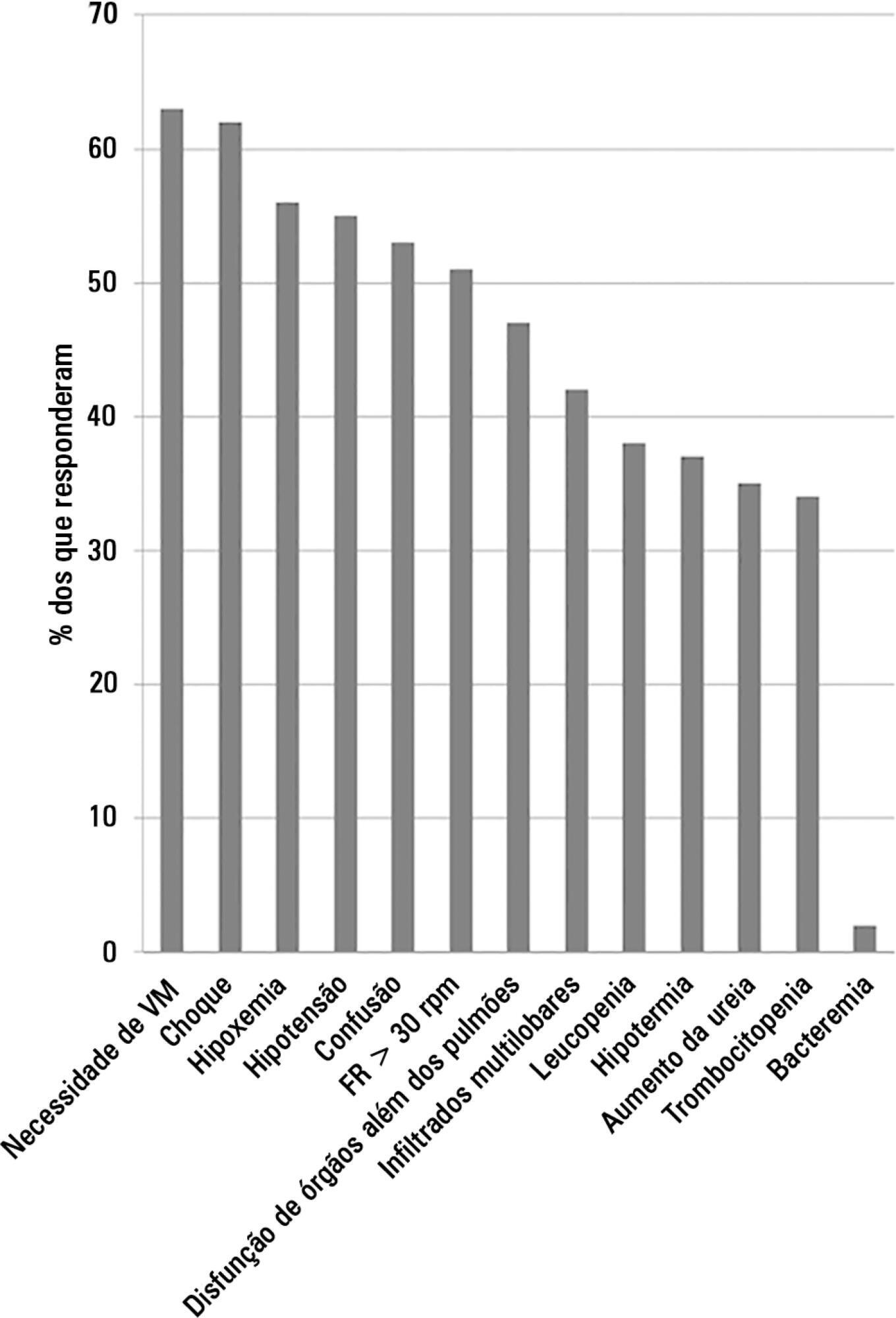
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):499-506
DOI 10.1590/S0103-507X2011000400016
Community-acquired pneumonia (CAP) is the most common infectious disease requiring admission to intensive care units (ICUs), and achieving an early and precise diagnosis of CAP remains a challenge. Biomarkers play an important role in improving clinical judgment in the emergency room and are adjuvant in evaluating treatment responses. Novel biomarkers, such as cortisol, pro-adrenomedullin and endothelin-1, have been shown to be associated with disease severity and short-term outcomes. This review article focuses on the clinical use of novel biomarkers, severity prediction and treatment monitoring as well as future directions of the field.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):499-506
DOI 10.1590/S0103-507X2011000400016
Community-acquired pneumonia (CAP) is the most common infectious disease requiring admission to intensive care units (ICUs), and achieving an early and precise diagnosis of CAP remains a challenge. Biomarkers play an important role in improving clinical judgment in the emergency room and are adjuvant in evaluating treatment responses. Novel biomarkers, such as cortisol, pro-adrenomedullin and endothelin-1, have been shown to be associated with disease severity and short-term outcomes. This review article focuses on the clinical use of novel biomarkers, severity prediction and treatment monitoring as well as future directions of the field.