Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Cassiano Teixeira"
We found (45) results for your search.Abstract
Rev Bras Ter Intensiva. 2019;31(4):592-593
DOI 10.5935/0103-507X.20190089
Abstract
Rev Bras Ter Intensiva. 2019;31(4):592-593
DOI 10.5935/0103-507X.20190089
Abstract
Rev Bras Ter Intensiva. 2019;31(4):598-599
DOI 10.5935/0103-507X.20190082
Abstract
Rev Bras Ter Intensiva. 2019;31(4):598-599
DOI 10.5935/0103-507X.20190082
Abstract
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
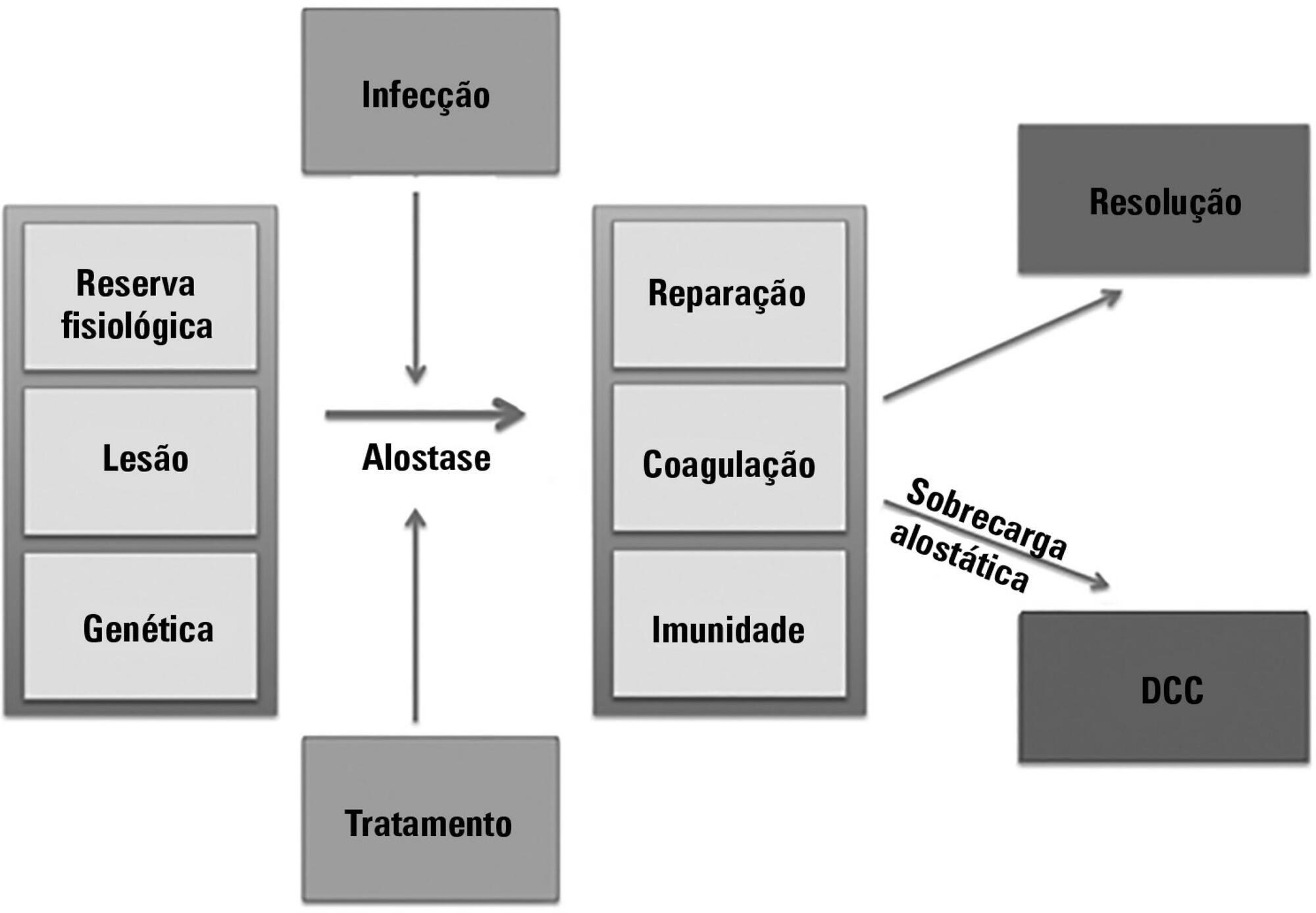
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
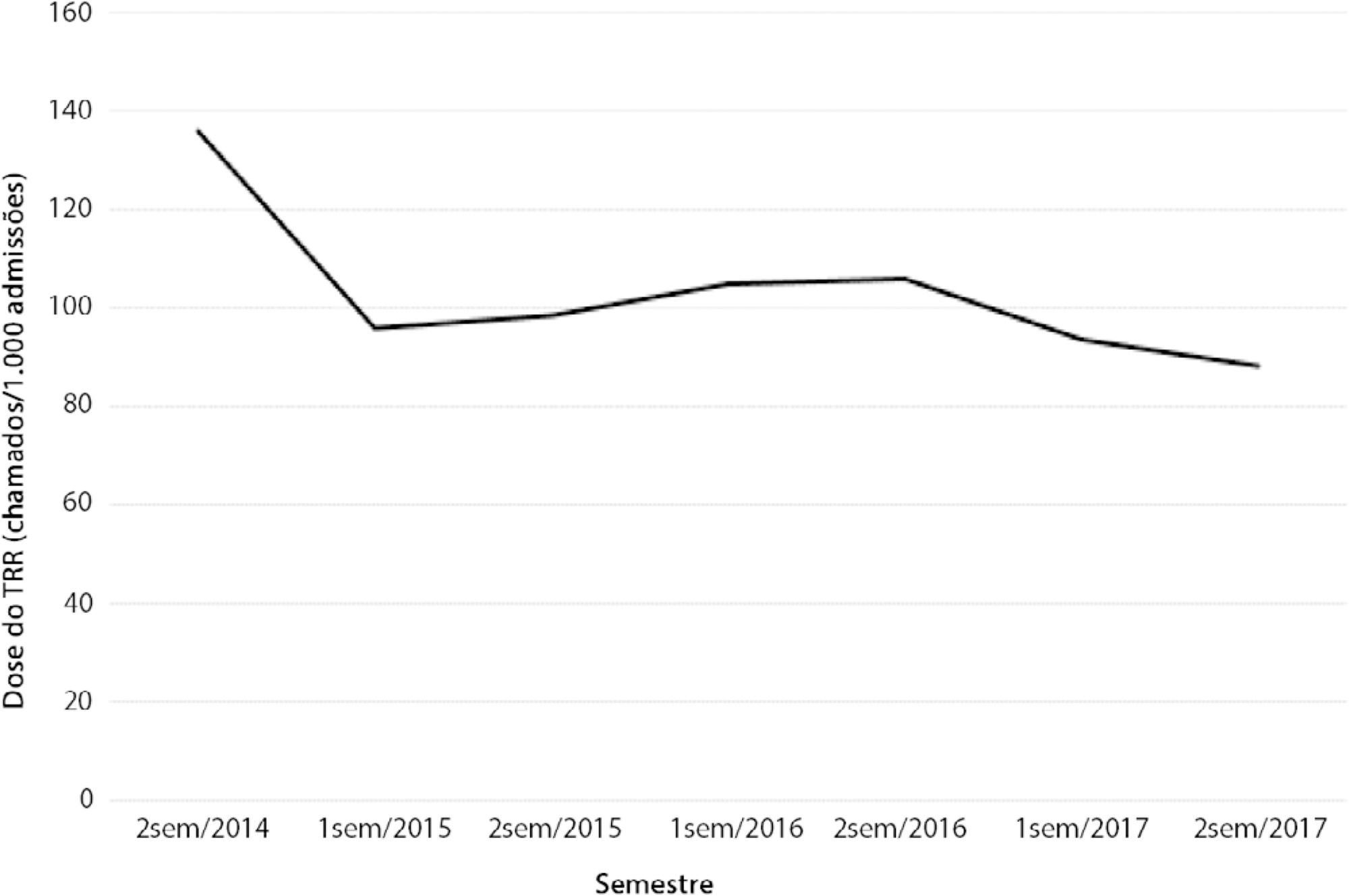
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.