
You searched for:"Marília Galvão Cruz"
We found (2) results for your search.-
Original Articles
Septic versus non-septic acute kidney injury in critically ill patients: characteristics and clinical outcomes
Rev Bras Ter Intensiva. 2014;26(4):384-391
Abstract
Original ArticlesSeptic versus non-septic acute kidney injury in critically ill patients: characteristics and clinical outcomes
Rev Bras Ter Intensiva. 2014;26(4):384-391
DOI 10.5935/0103-507X.20140059
Views0See moreObjective:
This study aimed to describe and compare the characteristics and clinical outcomes of patients with septic and non-septic acute kidney injury.
Methods:
This study evaluated an open cohort of 117 critically ill patients with acute kidney injury who were consecutively admitted to an intensive care unit, excluding patients with a history of advanced-stage chronic kidney disease, kidney transplantation, hospitalization or death in a period shorter than 24 hours. The presence of sepsis and in-hospital death were the exposure and primary variables in this study, respectively. A confounding analysis was performed using logistic regression.
Results:
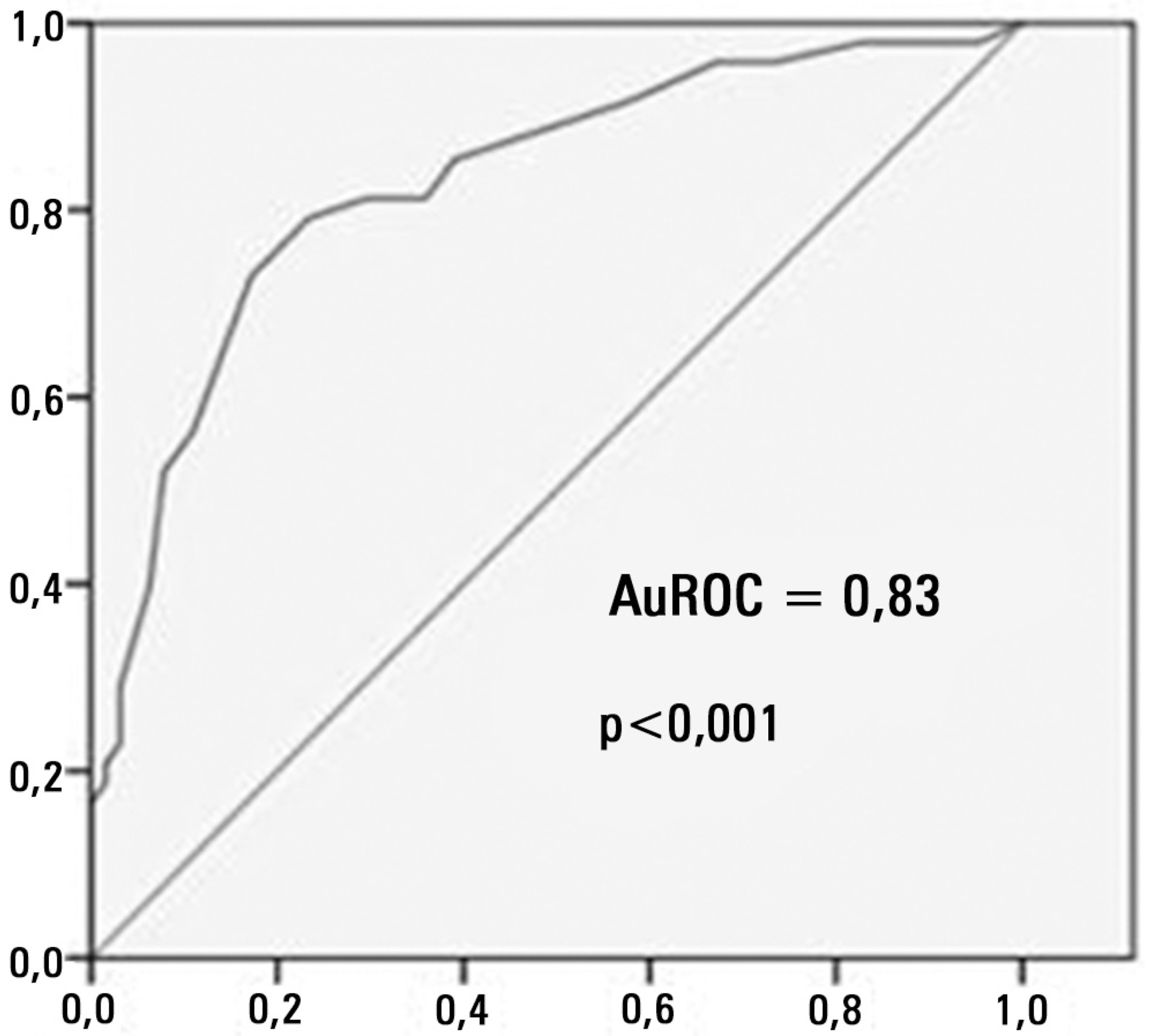
No significant differences were found between the mean ages of the groups with septic and non-septic acute kidney injury [65.30±21.27 years versus 66.35±12.82 years, respectively; p=0.75]. In the septic and non-septic acute kidney injury groups, a predominance of females (57.4% versus 52.4%, respectively; p=0.49) and Afro-descendants (81.5% versus 76.2%, respectively; p=0.49) was observed. Compared with the non-septic patients, the patients with sepsis had a higher mean Acute Physiology and Chronic Health Evaluation II score [21.73±7.26 versus 15.75±5.98; p<0.001)] and a higher mean water balance (p=0.001). Arterial hypertension (p=0.01) and heart failure (p<0.001) were more common in the non-septic patients. Septic acute kidney injury was associated with a greater number of patients who required dialysis (p=0.001) and a greater number of deaths (p<0.001); however, renal function recovery was more common in this group (p=0.01). Sepsis (OR: 3.88; 95%CI: 1.51-10.00) and an Acute Physiology and Chronic Health Evaluation II score >18.5 (OR: 9.77; 95%CI: 3.73-25.58) were associated with death in the multivariate analysis.
Conclusion:
Sepsis was an independent predictor of death. Significant differences were found between the characteristics and clinical outcomes of patients with septic versus non-septic acute kidney injury.
Views0

Abstract
Original ArticlesSeptic versus non-septic acute kidney injury in critically ill patients: characteristics and clinical outcomes
Rev Bras Ter Intensiva. 2014;26(4):384-391
DOI 10.5935/0103-507X.20140059
Views0See moreObjective:
This study aimed to describe and compare the characteristics and clinical outcomes of patients with septic and non-septic acute kidney injury.
Methods:
This study evaluated an open cohort of 117 critically ill patients with acute kidney injury who were consecutively admitted to an intensive care unit, excluding patients with a history of advanced-stage chronic kidney disease, kidney transplantation, hospitalization or death in a period shorter than 24 hours. The presence of sepsis and in-hospital death were the exposure and primary variables in this study, respectively. A confounding analysis was performed using logistic regression.
Results:
No significant differences were found between the mean ages of the groups with septic and non-septic acute kidney injury [65.30±21.27 years versus 66.35±12.82 years, respectively; p=0.75]. In the septic and non-septic acute kidney injury groups, a predominance of females (57.4% versus 52.4%, respectively; p=0.49) and Afro-descendants (81.5% versus 76.2%, respectively; p=0.49) was observed. Compared with the non-septic patients, the patients with sepsis had a higher mean Acute Physiology and Chronic Health Evaluation II score [21.73±7.26 versus 15.75±5.98; p<0.001)] and a higher mean water balance (p=0.001). Arterial hypertension (p=0.01) and heart failure (p<0.001) were more common in the non-septic patients. Septic acute kidney injury was associated with a greater number of patients who required dialysis (p=0.001) and a greater number of deaths (p<0.001); however, renal function recovery was more common in this group (p=0.01). Sepsis (OR: 3.88; 95%CI: 1.51-10.00) and an Acute Physiology and Chronic Health Evaluation II score >18.5 (OR: 9.77; 95%CI: 3.73-25.58) were associated with death in the multivariate analysis.
Conclusion:
Sepsis was an independent predictor of death. Significant differences were found between the characteristics and clinical outcomes of patients with septic versus non-septic acute kidney injury.
-
Original Articles
Comparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Rev Bras Ter Intensiva. 2013;25(4):290-296
Abstract
Original ArticlesComparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Rev Bras Ter Intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
Views7See moreObjective:
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study’s aim was to compare these criteria as predictors of mortality in critically ill patients.
Methods:
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student’s t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
Results:
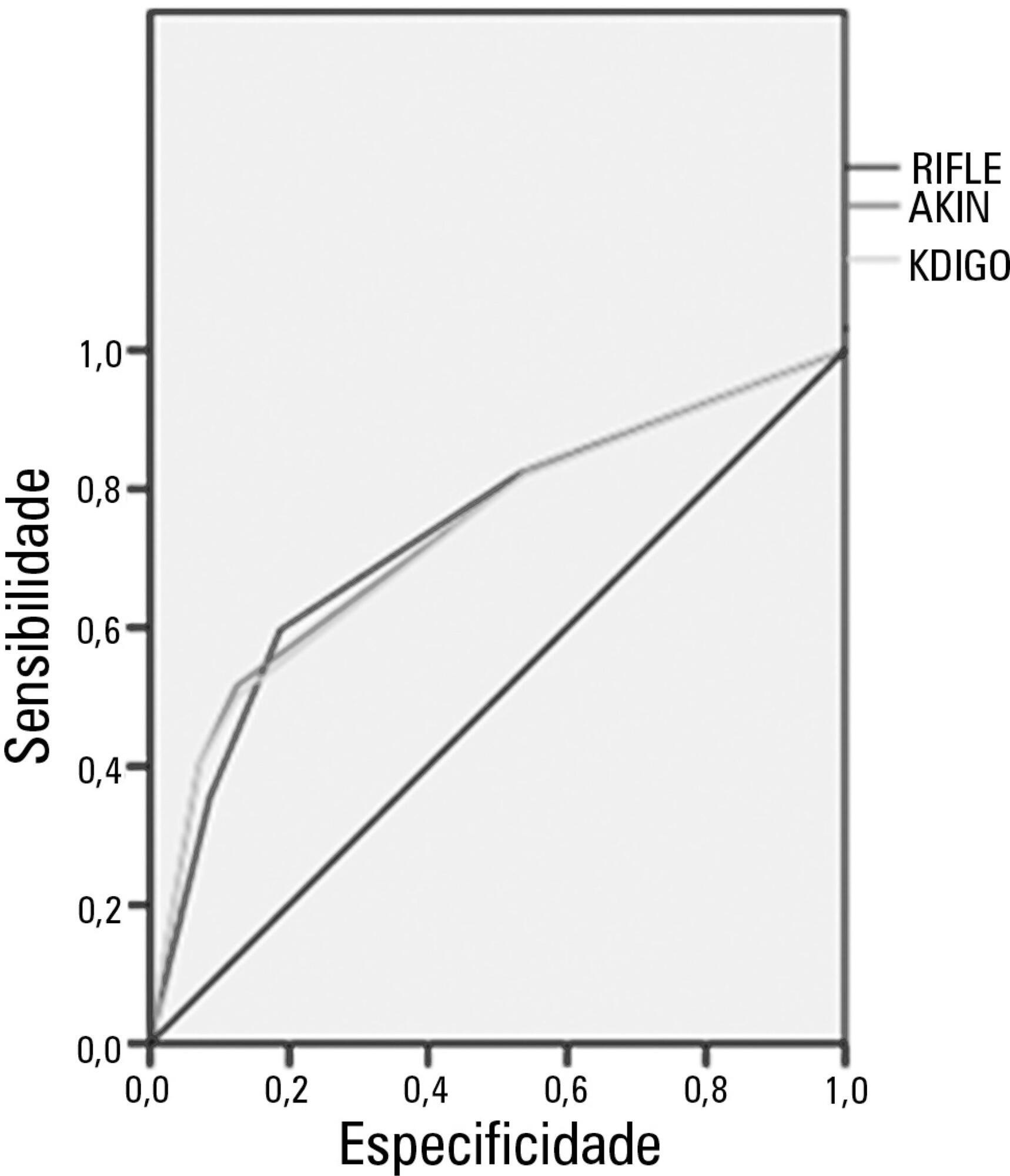
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
Conclusion:
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
Views7Abstract
Original ArticlesComparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Rev Bras Ter Intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
Views7See moreObjective:
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study’s aim was to compare these criteria as predictors of mortality in critically ill patients.
Methods:
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student’s t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
Results:
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
Conclusion:
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis Septic shock