Special Article Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(3):215-239
DOI 10.5935/0103-507X.20140034
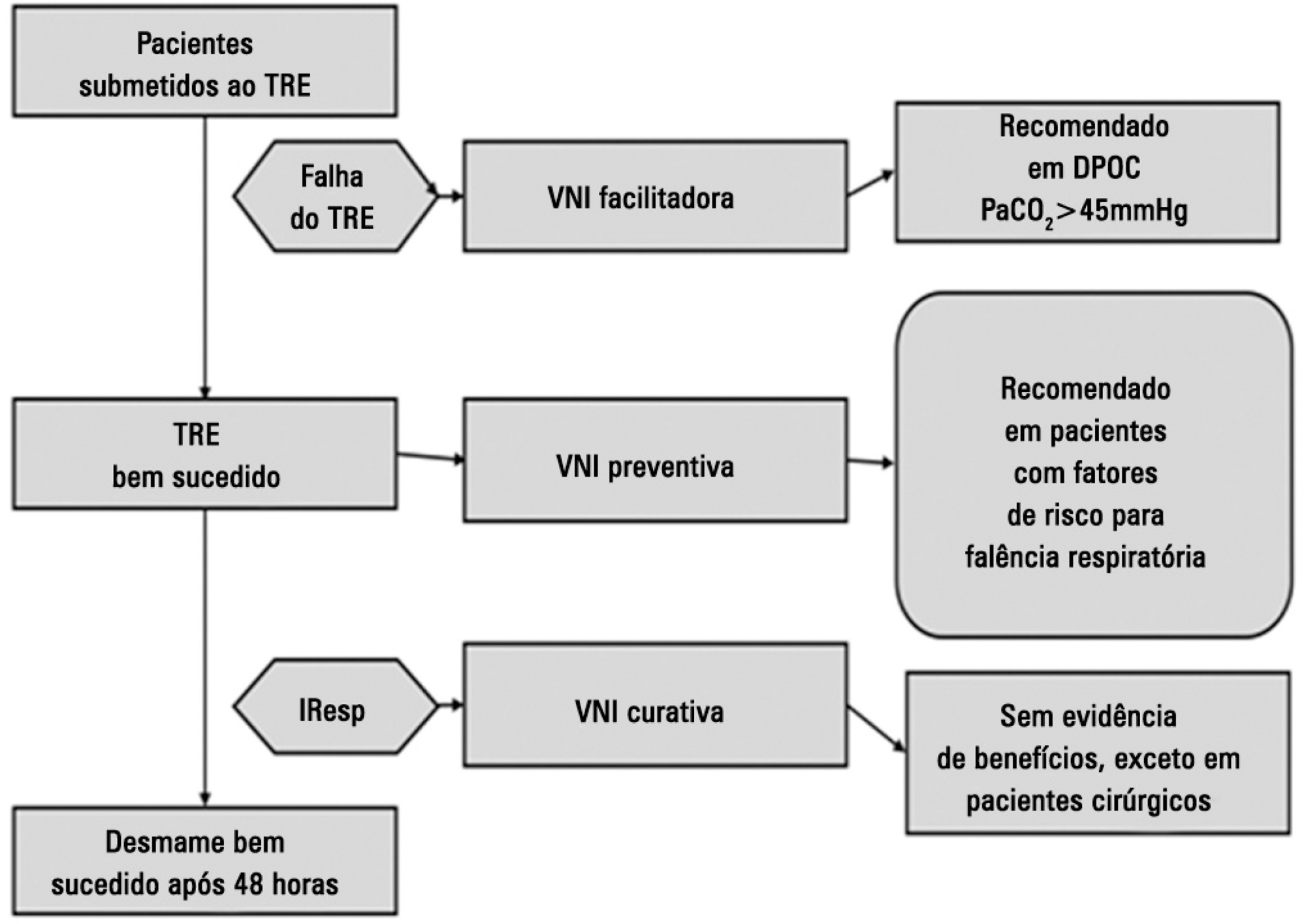
Perspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira - AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia - SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):215-239
DOI 10.5935/0103-507X.20140034
Perspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira - AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia - SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):240-252
DOI 10.5935/0103-507X.20140035
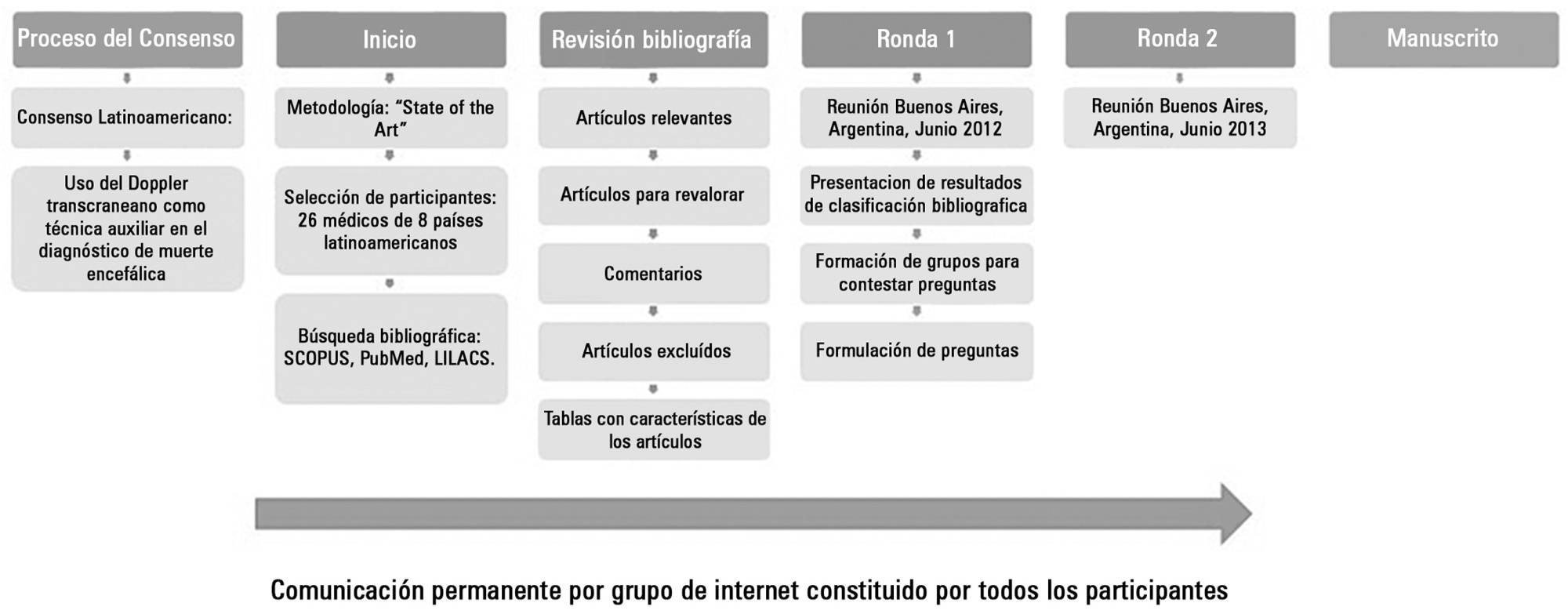
Transcranial Doppler evaluates cerebral hemodynamics in patients with brain injury and is a useful technical tool in diagnosing cerebral circulatory arrest, usually present in the brain-dead patient. This Latin American Consensus was formed by a group of 26 physicians experienced in the use of transcranial Doppler in the context of brain death. The purpose of this agreement was to make recommendations regarding the indications, technique, and interpretation of the study of transcranial ultrasonography in patients with a clinical diagnosis of brain death or in the patient whose clinical diagnosis presents difficulties; a working group was formed to enable further knowledge and to strengthen ties between Latin American physicians working on the same topic.
A review of the literature, concepts, and experiences were exchanged in two meetings and via the Internet. Questions about pathophysiology, equipment, techniques, findings, common problems, and the interpretation of transcranial Doppler in the context of brain death were answered. The basic consensus statements are the following: cerebral circulatory arrest is the final stage in the evolution of progressive intracranial hypertension, which is visualized with transcranial Doppler as a "pattern of cerebral circulatory arrest". The following are accepted as the standard of cerebral circulatory arrest: reverberant pattern, systolic spikes, and absence of previously demonstrated flow. Ultrasonography should be used - in acceptable hemodynamic conditions - in the anterior circulation bilaterally (middle cerebral artery) and in the posterior (basilar artery) territory. If no ultrasonographic images are found in any or all of these vessels, their proximal arteries are acceptable to be studied to look for a a pattern of cerebral circulatory arrest.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):240-252
DOI 10.5935/0103-507X.20140035
Transcranial Doppler evaluates cerebral hemodynamics in patients with brain injury and is a useful technical tool in diagnosing cerebral circulatory arrest, usually present in the brain-dead patient. This Latin American Consensus was formed by a group of 26 physicians experienced in the use of transcranial Doppler in the context of brain death. The purpose of this agreement was to make recommendations regarding the indications, technique, and interpretation of the study of transcranial ultrasonography in patients with a clinical diagnosis of brain death or in the patient whose clinical diagnosis presents difficulties; a working group was formed to enable further knowledge and to strengthen ties between Latin American physicians working on the same topic.
A review of the literature, concepts, and experiences were exchanged in two meetings and via the Internet. Questions about pathophysiology, equipment, techniques, findings, common problems, and the interpretation of transcranial Doppler in the context of brain death were answered. The basic consensus statements are the following: cerebral circulatory arrest is the final stage in the evolution of progressive intracranial hypertension, which is visualized with transcranial Doppler as a "pattern of cerebral circulatory arrest". The following are accepted as the standard of cerebral circulatory arrest: reverberant pattern, systolic spikes, and absence of previously demonstrated flow. Ultrasonography should be used - in acceptable hemodynamic conditions - in the anterior circulation bilaterally (middle cerebral artery) and in the posterior (basilar artery) territory. If no ultrasonographic images are found in any or all of these vessels, their proximal arteries are acceptable to be studied to look for a a pattern of cerebral circulatory arrest.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):77-80
DOI 10.5935/0103-507X.20130016
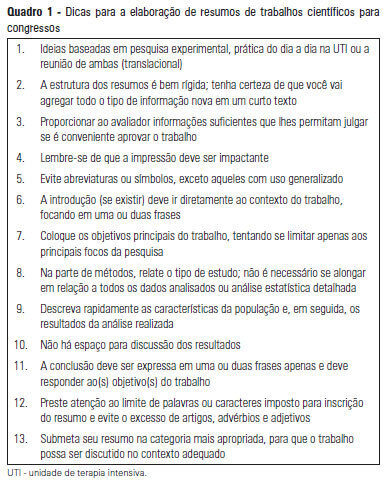
The presentation of study results is a key step in scientific research, and submitting an abstract to a meeting is often the first form of public communication. Meeting abstracts have a defined structure that is similar to abstracts for scientific articles, with an introduction, the objective, methods, results and conclusions. However, abstracts for meetings are not presented as part of a full article and, therefore, must contain the necessary and most relevant data. In this article, we detail their structure and include tips to make them technically correct.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):77-80
DOI 10.5935/0103-507X.20130016
The presentation of study results is a key step in scientific research, and submitting an abstract to a meeting is often the first form of public communication. Meeting abstracts have a defined structure that is similar to abstracts for scientific articles, with an introduction, the objective, methods, results and conclusions. However, abstracts for meetings are not presented as part of a full article and, therefore, must contain the necessary and most relevant data. In this article, we detail their structure and include tips to make them technically correct.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):81-86
Abstract
Rev Bras Ter Intensiva. 2013;25(2):81-86
Abstract
Rev Bras Ter Intensiva. 2013;25(1):3-5
DOI 10.1590/S0103-507X2013000100002
Abstract
Rev Bras Ter Intensiva. 2013;25(1):3-5
DOI 10.1590/S0103-507X2013000100002
Abstract
Abstract
Abstract
Rev Bras Ter Intensiva. 2013;25(4):265-269
DOI 10.5935/0103-507X.20130046
Abstract
Rev Bras Ter Intensiva. 2013;25(4):265-269
DOI 10.5935/0103-507X.20130046
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.