outcome Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2006;18(3):251-255
DOI 10.1590/S0103-507X2006000300006
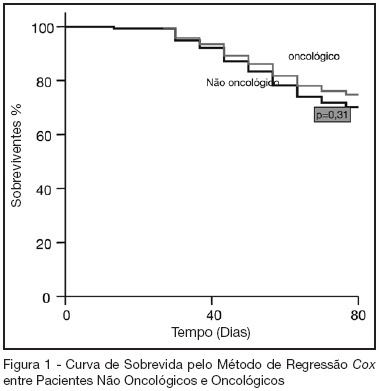
BACKGROUND AND OBJECTIVES: Oncologic diseases are conditions that have influence in the treatment offered to affected patients. The aim of this study was to compare hospitalar outcome of oncologic and non oncologic patients submitted to high risk elective surgery. METHODS: Prospective, observational cohort study realized in an ICU of a tertiary hospital during the period between 04/01/2005 and 07/31/2005. Demographic data, APACHE II and MODS scores and laboratorial and hemodynamic variables were collected and complications like re-intervention need for mechanical ventilation, red blood cell transfusions and pulmonary artery catheter use during the post-operative period were evaluated. All patients were followed until hospital discharge or death. T student and Mann Whitney tests were used to compare numerical variables. Chi-square test was used to compare categorical variables. A p < 0.05 was considered as significant. RESULTS: 119 patients were included in the study. 43 were oncologic and 76 were non-oncologic. 52.9% were female. Mean age was 65.1 ± 14.1 years. Mean APACHE II score was 16.5 ± 5.8 and MODS median was 3 (2-6). Median length of surgery was 5 (3.3-7) hours and ICU and hospital mortality were 10.9% and 25.2%, respectively. Oncologic patients had greater length of hospital stay and length of stay before surgery. These results were statistically significant. Hospital mortality of oncologic patients was not greater than non-oncologic patients (22.4% versus 30.2%, p = 0.32). CONCLUSIONS: In this series, oncologic patients submitted to high risk surgery had the same mortality rate as non-onconlogic patients with similar disease severity.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):251-255
DOI 10.1590/S0103-507X2006000300006
BACKGROUND AND OBJECTIVES: Oncologic diseases are conditions that have influence in the treatment offered to affected patients. The aim of this study was to compare hospitalar outcome of oncologic and non oncologic patients submitted to high risk elective surgery. METHODS: Prospective, observational cohort study realized in an ICU of a tertiary hospital during the period between 04/01/2005 and 07/31/2005. Demographic data, APACHE II and MODS scores and laboratorial and hemodynamic variables were collected and complications like re-intervention need for mechanical ventilation, red blood cell transfusions and pulmonary artery catheter use during the post-operative period were evaluated. All patients were followed until hospital discharge or death. T student and Mann Whitney tests were used to compare numerical variables. Chi-square test was used to compare categorical variables. A p < 0.05 was considered as significant. RESULTS: 119 patients were included in the study. 43 were oncologic and 76 were non-oncologic. 52.9% were female. Mean age was 65.1 ± 14.1 years. Mean APACHE II score was 16.5 ± 5.8 and MODS median was 3 (2-6). Median length of surgery was 5 (3.3-7) hours and ICU and hospital mortality were 10.9% and 25.2%, respectively. Oncologic patients had greater length of hospital stay and length of stay before surgery. These results were statistically significant. Hospital mortality of oncologic patients was not greater than non-oncologic patients (22.4% versus 30.2%, p = 0.32). CONCLUSIONS: In this series, oncologic patients submitted to high risk surgery had the same mortality rate as non-onconlogic patients with similar disease severity.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
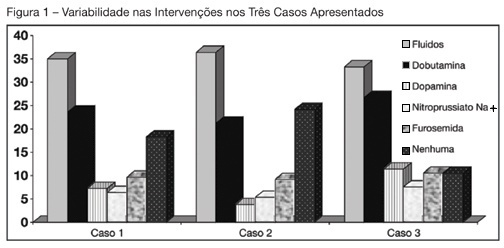
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
BACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
BACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):82-87
DOI 10.1590/S0103-507X2008000100013
BACKGROUND AND OBJECTIVES: Until the end of the previous century it remained controversial to admit cancer patients to the ICU for advanced-life-supporting therapy. However, over the past few years several centres over the world have shown that it is possible to achieve a meaningful survival in these patients. The aim of this review is to focus on the improvement in outcome that has been achieved over the past two decades in critically ill cancer patients. CONTENTS: We performed a MEDLINE search (period of 1980 to November 2007) to identify full-text English language publications on critically ill patients with solid tumors or hematological malignancies with particular interest for the outcome and treatment. Major MESH search terms included; cancer, solid tumor, hematologic or hematological malignancies, immunosupression, ICU, ventilation, organ failure, sepsis and infection. Additional studies were identified through a manual search of citations from retrieved articles. CONCLUSIONS: In this review, we first focus on the grim prognosis in the past, subsequently we discuss the improvements in outcome over the past few years across subgroups of cancer patients with increasing degree of severity of illness, and finally, we focus on the value of non-invasive ventilation since it is considered the initial ventilatory strategy in these patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):82-87
DOI 10.1590/S0103-507X2008000100013
BACKGROUND AND OBJECTIVES: Until the end of the previous century it remained controversial to admit cancer patients to the ICU for advanced-life-supporting therapy. However, over the past few years several centres over the world have shown that it is possible to achieve a meaningful survival in these patients. The aim of this review is to focus on the improvement in outcome that has been achieved over the past two decades in critically ill cancer patients. CONTENTS: We performed a MEDLINE search (period of 1980 to November 2007) to identify full-text English language publications on critically ill patients with solid tumors or hematological malignancies with particular interest for the outcome and treatment. Major MESH search terms included; cancer, solid tumor, hematologic or hematological malignancies, immunosupression, ICU, ventilation, organ failure, sepsis and infection. Additional studies were identified through a manual search of citations from retrieved articles. CONCLUSIONS: In this review, we first focus on the grim prognosis in the past, subsequently we discuss the improvements in outcome over the past few years across subgroups of cancer patients with increasing degree of severity of illness, and finally, we focus on the value of non-invasive ventilation since it is considered the initial ventilatory strategy in these patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):396-401
DOI 10.1590/S0103-507X2006000400013
BACKGROUND AND OBJECTIVES: Cardiac arrest is a state of severe cerebral perfusion deficit. Patients recovering from a cardiopulmonary resuscitation are at great risk of subsequent death or incapacitating neurologic injury, including persistent vegetative state. The early definition of prognosis for these patients has ethical and economic implications. The main purpose of this manuscript was to review the prognostic value of serum Neuron-Specific Enolase (NSE) in predicting outcomes in patients early after a cardiac arrest. CONTENTS: Severe neurologic disability is the most feared complication after a cardiac arrest. Many studies are trying to find prognostic markers that can be associated with outcomes in patients surviving a cardiac arrest. Biochemical markers of neuronal injury seem to be promising in this scenario. Therefore, NSE levels have been studied in patients after a cardiac arrest and high enzyme levels suggest more extensive brain damage and are associated with unfavorable clinical outcomes. CONCLUSIONS: Outcome after a cardiac arrest is mostly determined by the degree of hypoxic brain damage and early determinations of serum NSE level can be a valuable ancillary method for assessing outcome in these patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):396-401
DOI 10.1590/S0103-507X2006000400013
BACKGROUND AND OBJECTIVES: Cardiac arrest is a state of severe cerebral perfusion deficit. Patients recovering from a cardiopulmonary resuscitation are at great risk of subsequent death or incapacitating neurologic injury, including persistent vegetative state. The early definition of prognosis for these patients has ethical and economic implications. The main purpose of this manuscript was to review the prognostic value of serum Neuron-Specific Enolase (NSE) in predicting outcomes in patients early after a cardiac arrest. CONTENTS: Severe neurologic disability is the most feared complication after a cardiac arrest. Many studies are trying to find prognostic markers that can be associated with outcomes in patients surviving a cardiac arrest. Biochemical markers of neuronal injury seem to be promising in this scenario. Therefore, NSE levels have been studied in patients after a cardiac arrest and high enzyme levels suggest more extensive brain damage and are associated with unfavorable clinical outcomes. CONCLUSIONS: Outcome after a cardiac arrest is mostly determined by the degree of hypoxic brain damage and early determinations of serum NSE level can be a valuable ancillary method for assessing outcome in these patients.