Influenza A virus Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
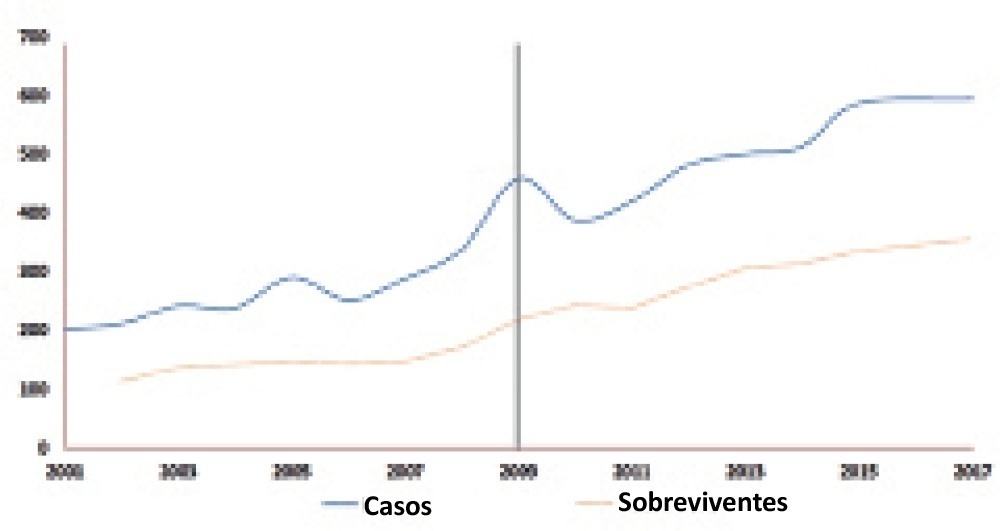
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
In the 2014 - 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 - 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
In the 2014 - 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 - 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.

Abstract
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
OBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student's t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
OBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student's t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.