Hypotension Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
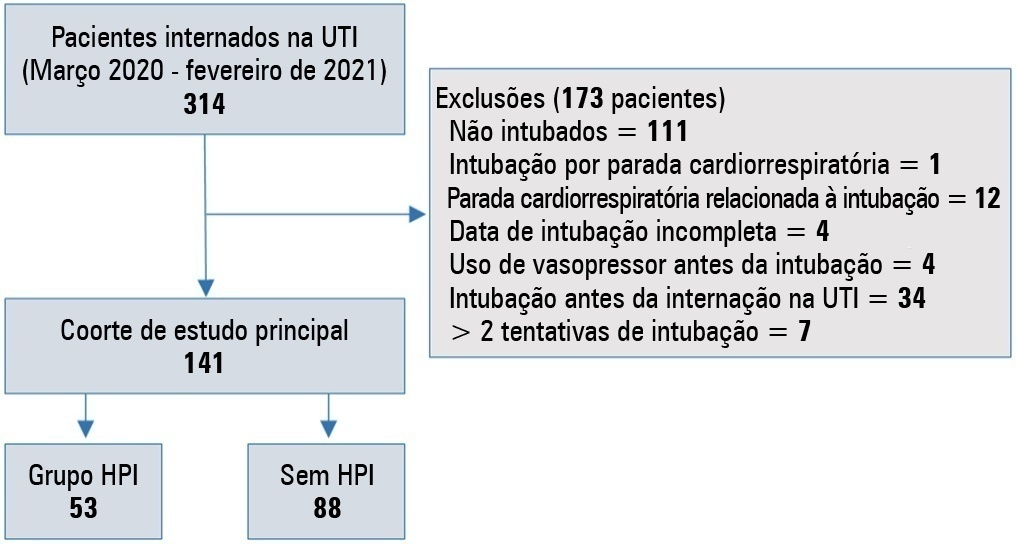
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 - 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 - 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 - 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 - 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):423-428
DOI 10.5935/0103-507X.20180060
To evaluate the short-term evolution of patients with septic shock refractory to norepinephrine treated with vasopressin in an intensive care unit of a university hospital.
An unmatched retrospective study (case series) was performed. Clinical, laboratory, and anthropometric data were collected from patients who received vasopressin infusion for treatment of catecholamine-refractory shock from December 2014 to June 2016. For the assessment of severity, APACHE II and SOFA scores were used. The main outcome was mortality at 3 and 30 days.
A total of 80 patients were included, of which 60% were male. In 86.3% of the cases, APACHE II was observed in the highest ranges (> 20). The 30-day mortality was 86.2%, and 75% of the patients died within 72 hours after starting vasopressin.
The series evaluated had high mortality in the first 72 hours of treatment with vasopressin. The use of vasopressin in patients who are refractory to norepinephrine had little or no impact on mortality. It was not possible to exclude the possibility that the high mortality in the present study was linked to the relatively late onset (after established refractoriness of norepinephrine) of vasopressin; this hypothesis should be further evaluated in a randomized study.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):423-428
DOI 10.5935/0103-507X.20180060
To evaluate the short-term evolution of patients with septic shock refractory to norepinephrine treated with vasopressin in an intensive care unit of a university hospital.
An unmatched retrospective study (case series) was performed. Clinical, laboratory, and anthropometric data were collected from patients who received vasopressin infusion for treatment of catecholamine-refractory shock from December 2014 to June 2016. For the assessment of severity, APACHE II and SOFA scores were used. The main outcome was mortality at 3 and 30 days.
A total of 80 patients were included, of which 60% were male. In 86.3% of the cases, APACHE II was observed in the highest ranges (> 20). The 30-day mortality was 86.2%, and 75% of the patients died within 72 hours after starting vasopressin.
The series evaluated had high mortality in the first 72 hours of treatment with vasopressin. The use of vasopressin in patients who are refractory to norepinephrine had little or no impact on mortality. It was not possible to exclude the possibility that the high mortality in the present study was linked to the relatively late onset (after established refractoriness of norepinephrine) of vasopressin; this hypothesis should be further evaluated in a randomized study.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):416-420
DOI 10.5935/0103-507X.20140064
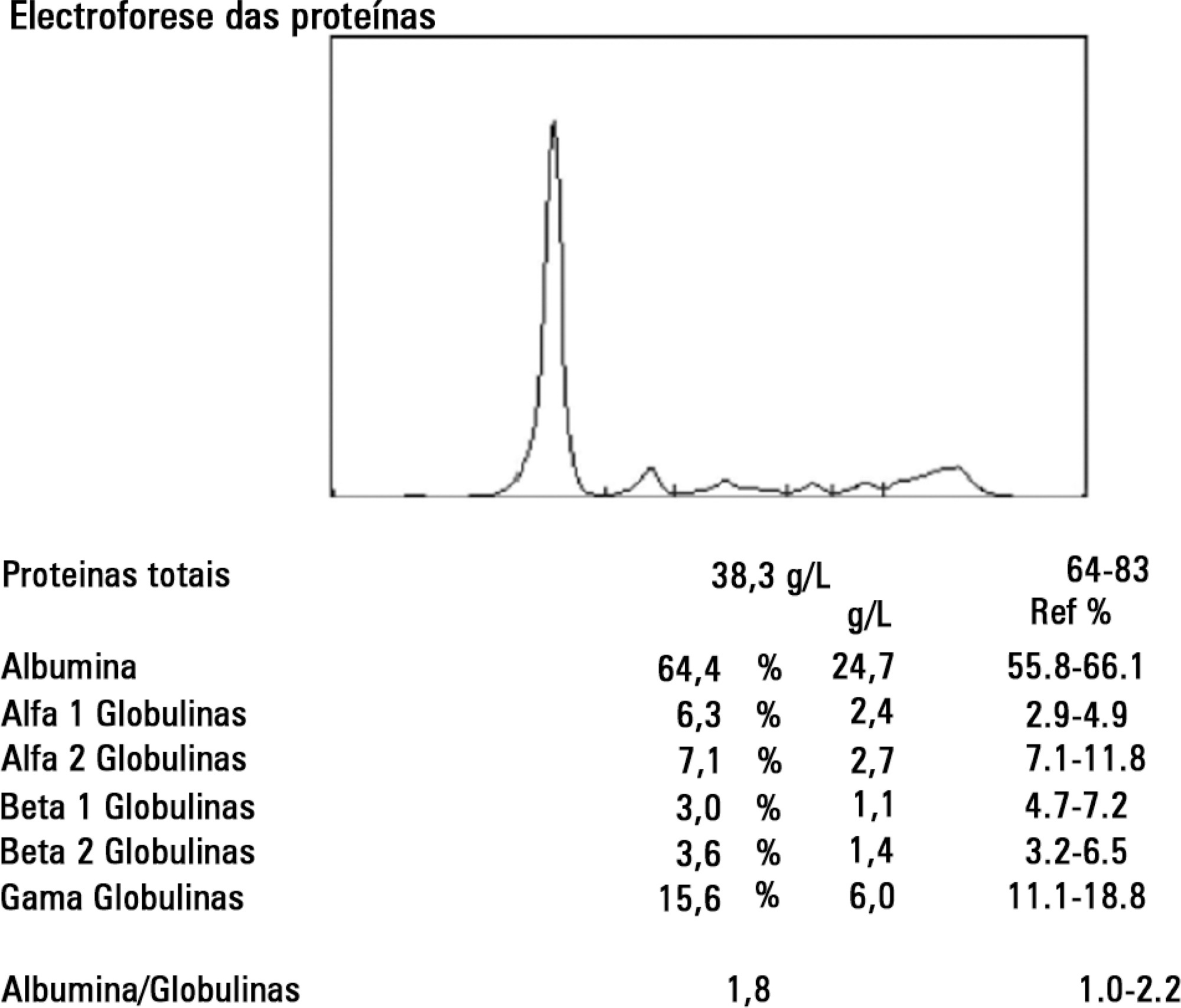
The authors report a rare case of shock in a patient without significant clinical history, admitted to the intensive care unit for suspected septic shock. The patient was initially treated with fluid therapy without improvement. A hypothesis of systemic capillary leak syndrome was postulated following the confirmation of severe hypoalbuminemia, hypotension, and hemoconcentration - a combination of three symptoms typical of the disease. The authors discussed the differential diagnosis and also conducted a review of the diagnosis and treatment of the disease.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):416-420
DOI 10.5935/0103-507X.20140064
The authors report a rare case of shock in a patient without significant clinical history, admitted to the intensive care unit for suspected septic shock. The patient was initially treated with fluid therapy without improvement. A hypothesis of systemic capillary leak syndrome was postulated following the confirmation of severe hypoalbuminemia, hypotension, and hemoconcentration - a combination of three symptoms typical of the disease. The authors discussed the differential diagnosis and also conducted a review of the diagnosis and treatment of the disease.