burns Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(2):276-281
DOI 10.5935/0103-507X.20210035
To evaluate serum uteroglobin-related protein 1 expression early after smoke inhalation injuries and its association with the severity of inhalation injury in burned patients.
Smoke or chemical inhalation injury is associated with morbidity and mortality. The consequences of inhalation result from an inflammatory response. Uteroglobin-related protein 1 is an anti-inflammatory protein and may improve lung inflammation. We hypothesized that uteroglobin-related protein 1 levels could reflect disease severity and predict outcome in patients with inhalation injury. Sixteen patients diagnosed with acute respiratory distress syndrome secondary to smoke inhalation injury were prospectively included in the study. Plasma was collected upon intensive care unit admission and within 24 hours of the inhalation injury. Bronchoscopies were carried out in all patients to assess the severity of inhalation injury within 72 hours. Uteroglobin-related protein 1 plasma levels were determined in duplicate with enzyme-linked immunosorbent assay.
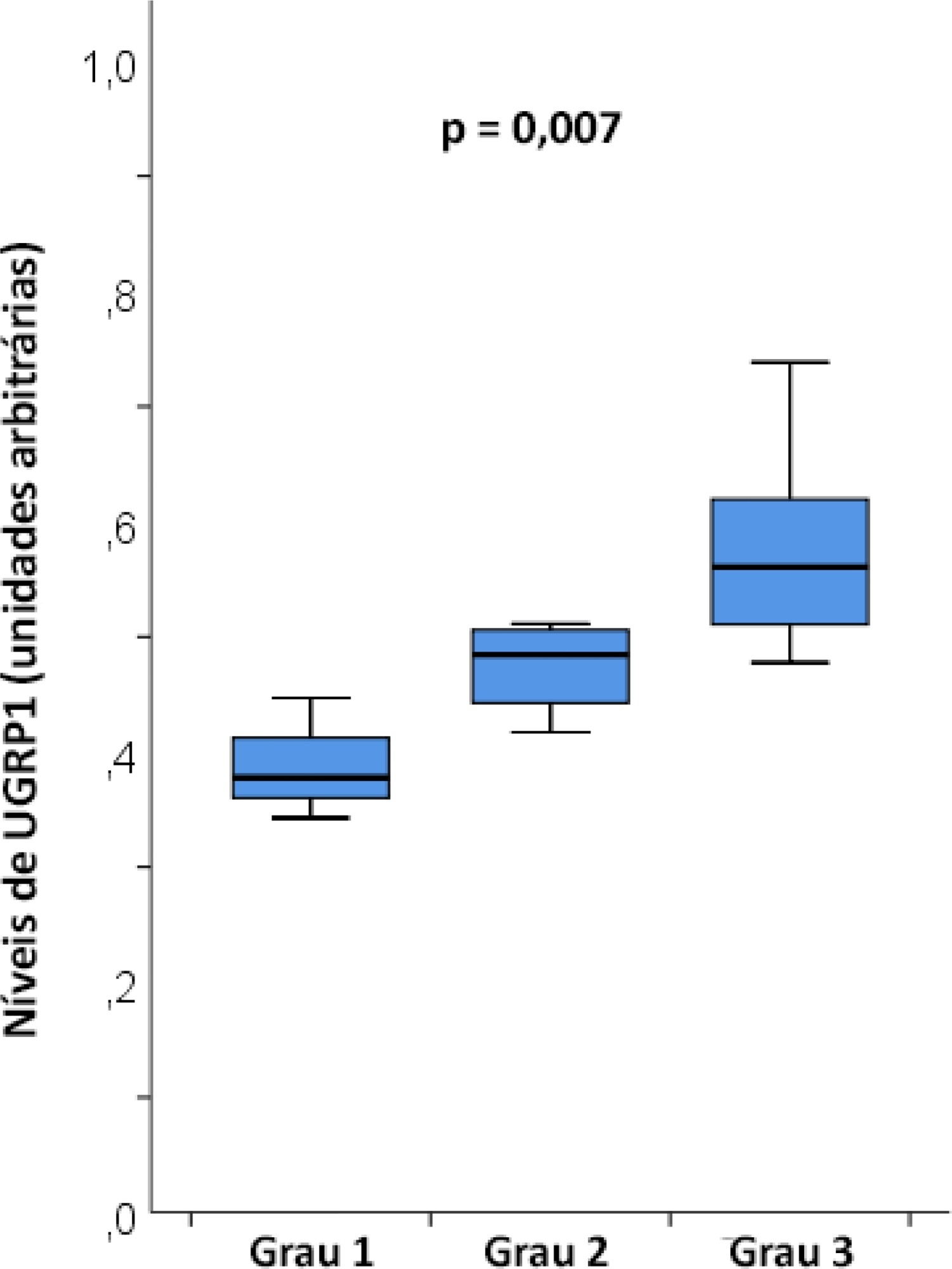
The mean age was 23 ± 5 years, and the inhalation injury distribution was as follows: three of grade 1, four of grade 2, and nine of grade 3. The level of uteroglobin-related protein 1 was related to inhalation severity (grade 1: 0.389 ± 0.053 arbitrary units versus grade 2: 0.474 ± 0.0423 arbitrary units versus grade 3: 0.580 ± 0.094 arbitrary units; p = 0.007).
Plasma levels of uteroglobin-related protein 1 are associated with the degree of lung inhalation injury.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):276-281
DOI 10.5935/0103-507X.20210035
To evaluate serum uteroglobin-related protein 1 expression early after smoke inhalation injuries and its association with the severity of inhalation injury in burned patients.
Smoke or chemical inhalation injury is associated with morbidity and mortality. The consequences of inhalation result from an inflammatory response. Uteroglobin-related protein 1 is an anti-inflammatory protein and may improve lung inflammation. We hypothesized that uteroglobin-related protein 1 levels could reflect disease severity and predict outcome in patients with inhalation injury. Sixteen patients diagnosed with acute respiratory distress syndrome secondary to smoke inhalation injury were prospectively included in the study. Plasma was collected upon intensive care unit admission and within 24 hours of the inhalation injury. Bronchoscopies were carried out in all patients to assess the severity of inhalation injury within 72 hours. Uteroglobin-related protein 1 plasma levels were determined in duplicate with enzyme-linked immunosorbent assay.
The mean age was 23 ± 5 years, and the inhalation injury distribution was as follows: three of grade 1, four of grade 2, and nine of grade 3. The level of uteroglobin-related protein 1 was related to inhalation severity (grade 1: 0.389 ± 0.053 arbitrary units versus grade 2: 0.474 ± 0.0423 arbitrary units versus grade 3: 0.580 ± 0.094 arbitrary units; p = 0.007).
Plasma levels of uteroglobin-related protein 1 are associated with the degree of lung inhalation injury.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):333-337
DOI 10.5935/0103-507X.20180045
To analyze the characteristics and outcomes of children hospitalized for burns in a pediatric trauma intensive care unit for burn patients.
An observational study was conducted through the retrospective analysis of children (< 16 years) admitted to the pediatric trauma intensive care unit for burn victims between January 2013 and December 2015. Sociodemographic and clinical variables were analyzed including the causal agent, burned body surface, presence of inhalation injury, length of hospital stay and mortality.
The study analyzed a sum of 140 patients; 61.8% were male, with a median age of 24 months and an overall mortality of 5%. The main cause of burns was scalding (51.4%), followed by accidents involving fire (38.6%) and electric shock (6.4%). Mechanical ventilation was used in 20.7% of the cases. Associated inhalation injury presented a relative risk of 6.1 (3.5 - 10.7) of needing ventilatory support and a relative risk of mortality of 14.1 (2.9 - 68.3) compared to patients without this associated injury. A significant connection was found between burned body surface and mortality (p < 0.002), reaching 80% in patients with a burned area greater than 50%. Patients who died had a significantly higher Tobiasen Abbreviated Burn Severity Index than survivors (9.6 ± 2.2 versus 4.4 ± 1.1; p < 0.001). A Tobiasen Abbreviated Burn Severity Index ≥ 7 represented a relative risk of death of 68.4 (95%CI 9.1 - 513.5).
Scalding burns are quite frequent and are associated with high morbidity. Mortality is associated with the amount of burned body surface and the presence of inhalation injury. Special emphasis should be given to accidents involving fire, reinforcing proper diagnosis and treatment of inhalation injury.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):333-337
DOI 10.5935/0103-507X.20180045
To analyze the characteristics and outcomes of children hospitalized for burns in a pediatric trauma intensive care unit for burn patients.
An observational study was conducted through the retrospective analysis of children (< 16 years) admitted to the pediatric trauma intensive care unit for burn victims between January 2013 and December 2015. Sociodemographic and clinical variables were analyzed including the causal agent, burned body surface, presence of inhalation injury, length of hospital stay and mortality.
The study analyzed a sum of 140 patients; 61.8% were male, with a median age of 24 months and an overall mortality of 5%. The main cause of burns was scalding (51.4%), followed by accidents involving fire (38.6%) and electric shock (6.4%). Mechanical ventilation was used in 20.7% of the cases. Associated inhalation injury presented a relative risk of 6.1 (3.5 - 10.7) of needing ventilatory support and a relative risk of mortality of 14.1 (2.9 - 68.3) compared to patients without this associated injury. A significant connection was found between burned body surface and mortality (p < 0.002), reaching 80% in patients with a burned area greater than 50%. Patients who died had a significantly higher Tobiasen Abbreviated Burn Severity Index than survivors (9.6 ± 2.2 versus 4.4 ± 1.1; p < 0.001). A Tobiasen Abbreviated Burn Severity Index ≥ 7 represented a relative risk of death of 68.4 (95%CI 9.1 - 513.5).
Scalding burns are quite frequent and are associated with high morbidity. Mortality is associated with the amount of burned body surface and the presence of inhalation injury. Special emphasis should be given to accidents involving fire, reinforcing proper diagnosis and treatment of inhalation injury.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
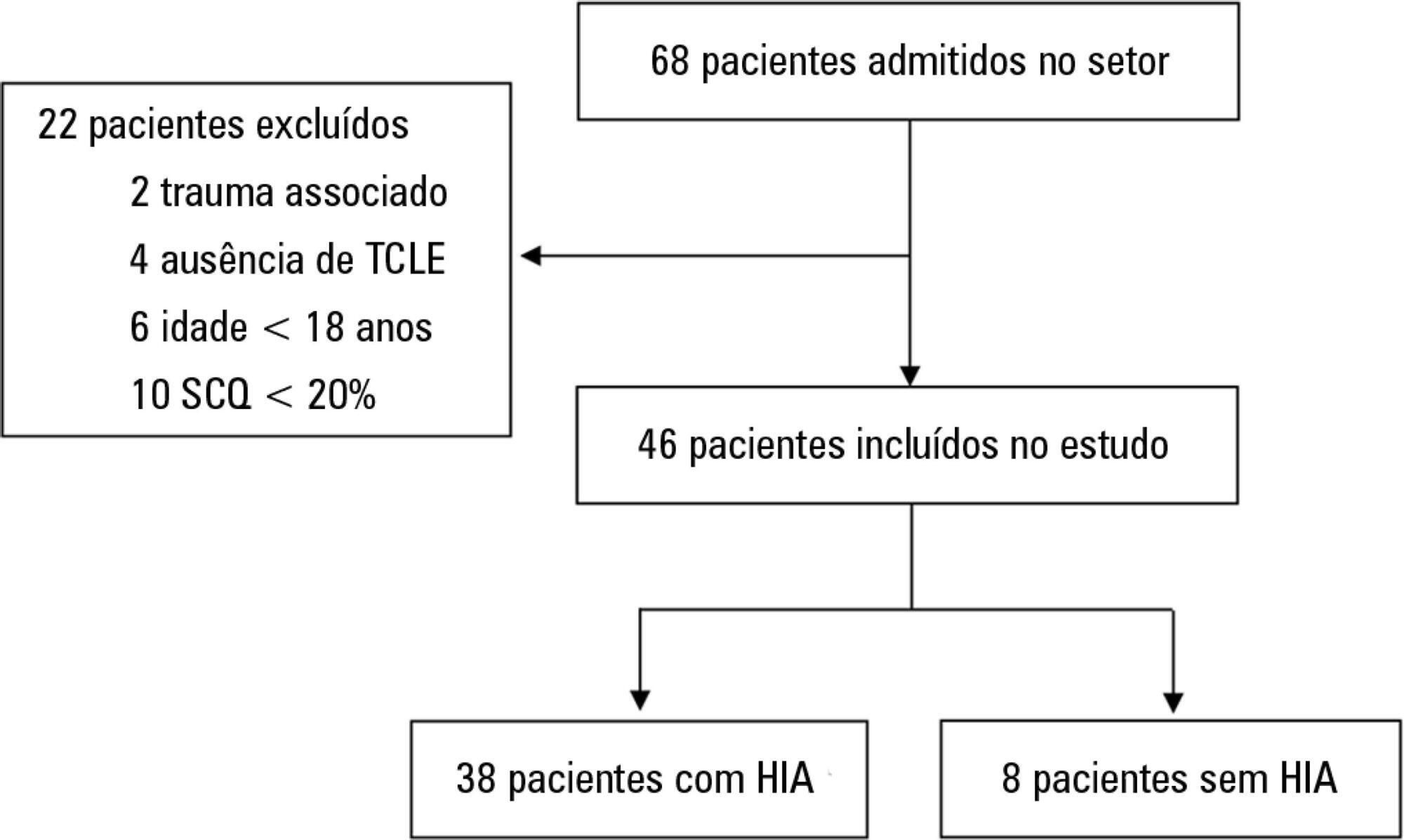
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
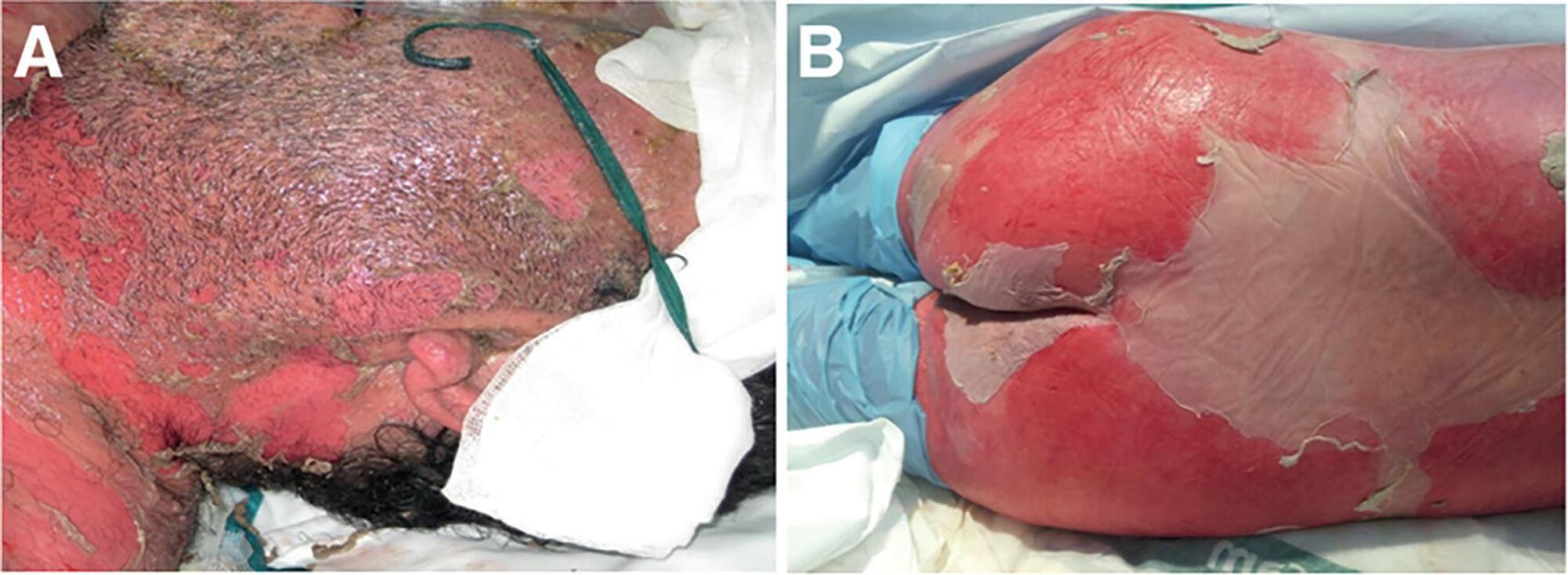
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):200-203
DOI 10.1590/S0103-507X2006000200015
BACKGROUND AND OBJECTIVES: To assess the use of recombinant human growth hormone (rhGH) in pediatric patients with hypercatabolic state in the pediatric intensive care unit. METHODS: We searched the databases of MedLine (1990 to 2005), LILACS (1990 to 2005), OVID (1990 to 2006) and EMBASE (1990 to 2005). Randomized controlled trials in pediatric patients using rhGH for hypercatabolic state (burns, sepsis) were selected. Intervention included rhGH therapy versus placebo. Data were extracted in duplicate and independently. Meta-analyses were performed using the software Review Manager statistic tools, with Mantel-Haenzel method for dichotomous outcomes and inverse variance method for continuous. RESULTS: There were evidences that rhGH in burned pediatric patients can reduce exogenous albumin requirement, with a improvement in Lean Body Mass, and accelerate site-donor wound healing, with no effects on mortality. Possibly can reduce the length of hospital stay. Hyperglycemia was the most frequently reported adverse event. CONCLUSIONS: This review suggests that the early application of rhGH to standard treatment in pediatric severe burned patients has the potential to improve some aspects from outcome. At this time, although the literature does not support routine rhGH for pediatric burn patients, consideration should be given to its use in this group, at least as an aim for further research. For use in septic patients, no proper statement can be done.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):200-203
DOI 10.1590/S0103-507X2006000200015
BACKGROUND AND OBJECTIVES: To assess the use of recombinant human growth hormone (rhGH) in pediatric patients with hypercatabolic state in the pediatric intensive care unit. METHODS: We searched the databases of MedLine (1990 to 2005), LILACS (1990 to 2005), OVID (1990 to 2006) and EMBASE (1990 to 2005). Randomized controlled trials in pediatric patients using rhGH for hypercatabolic state (burns, sepsis) were selected. Intervention included rhGH therapy versus placebo. Data were extracted in duplicate and independently. Meta-analyses were performed using the software Review Manager statistic tools, with Mantel-Haenzel method for dichotomous outcomes and inverse variance method for continuous. RESULTS: There were evidences that rhGH in burned pediatric patients can reduce exogenous albumin requirement, with a improvement in Lean Body Mass, and accelerate site-donor wound healing, with no effects on mortality. Possibly can reduce the length of hospital stay. Hyperglycemia was the most frequently reported adverse event. CONCLUSIONS: This review suggests that the early application of rhGH to standard treatment in pediatric severe burned patients has the potential to improve some aspects from outcome. At this time, although the literature does not support routine rhGH for pediatric burn patients, consideration should be given to its use in this group, at least as an aim for further research. For use in septic patients, no proper statement can be done.