
You searched for:"Arnaldo Dubin"
We found (12) results for your search.-
Original Article
Lack of agreement between different observers and methods in the measurement of capillary refill time in healthy volunteers: an observational study
Rev Bras Ter Intensiva. 2014;26(3):269-276
Abstract
Original ArticleLack of agreement between different observers and methods in the measurement of capillary refill time in healthy volunteers: an observational study
Rev Bras Ter Intensiva. 2014;26(3):269-276
DOI 10.5935/0103-507X.20140038
Views0See moreObjective:
Peripheral perfusion abnormalities are relevant manifestations of shock. Capillary refill time is commonly used for their evaluation. However, the reproducibility of capillary refill time measurements and their correlation with other variables of peripheral perfusion, have not been comprehensively evaluated. Our goal was to determine, in healthy volunteers, the agreement between different methods of capillary refill time quantification and different observers, as well as their correlation with other markers of peripheral perfusion.
Methods:
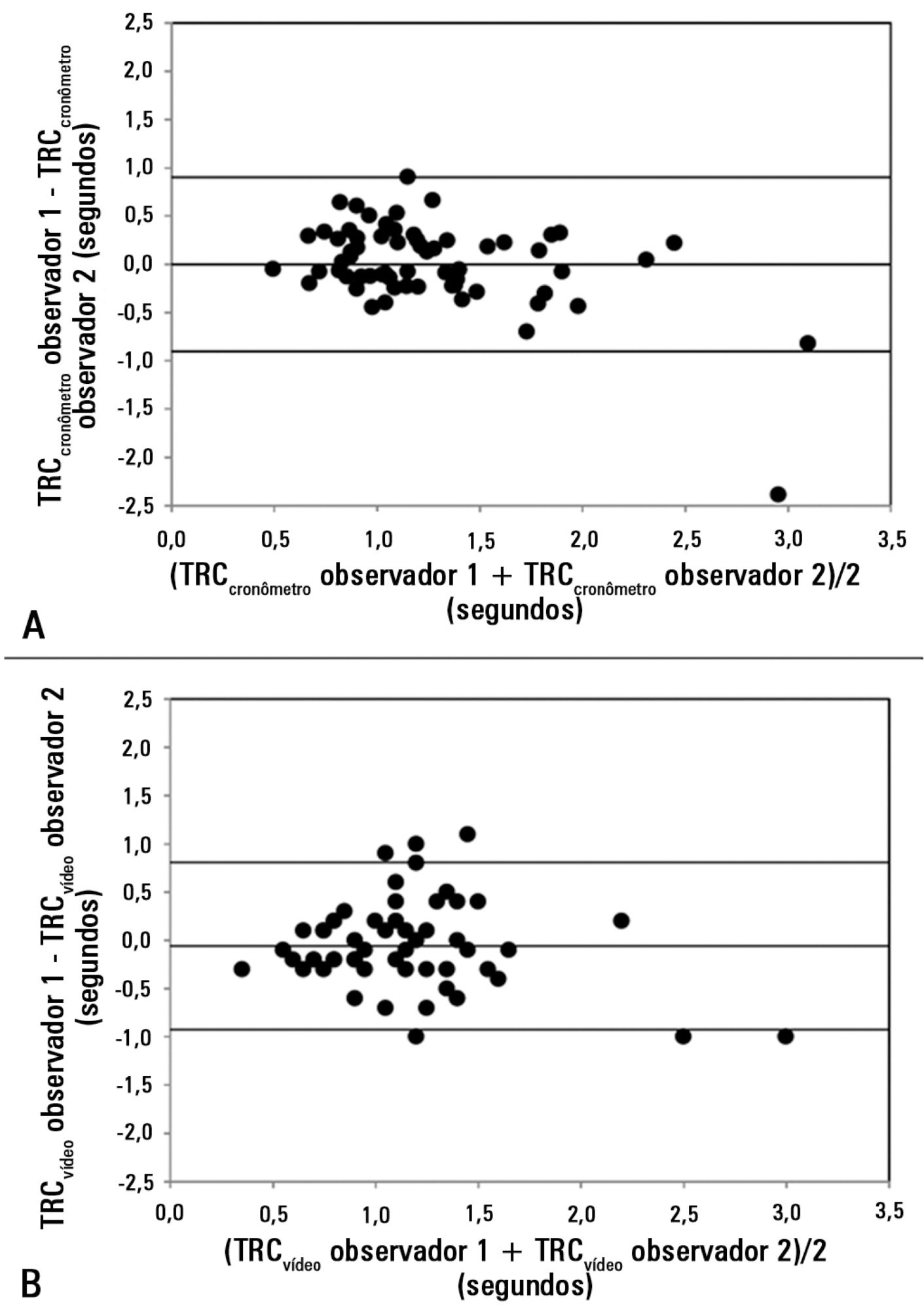
We studied 63 healthy volunteers. Two observers measured capillary refill time by means of two methods, direct view (CRTchronometer) and video analysis (CRTvideo). We also measured perfusion index (PI) derived from pulse plethysmography and finger pad temperature (Tºperipheral). The agreement between observers and methods was assessed using the Bland and Altman method. Correlations were calculated using Pearson’s correlation. A p-value<0.05 was considered significant.
Results:
The 95% limits of agreement between the two observers were 1.9 sec for CRTchronometer and 1.7 sec for CRTvideo. The 95% limits of agreement between CRTchronometer and CRTvideo were 1.7 sec for observer 1 and 2.3 sec for observer 2. Measurements of CRTchronometer performed by the two observers were correlated with Tºperipheral. Measurements of CRTvideo performed by the two observers were correlated with Tºperipheral and perfusion index.
Conclusion:
In healthy volunteers, measurements of capillary refill time performed by either different observers or different methods showed poor agreement. Nevertheless, capillary refill time still reflected peripheral perfusion as shown by its correlation with objective variables of peripheral perfusion.
Views0

Abstract
Original ArticleLack of agreement between different observers and methods in the measurement of capillary refill time in healthy volunteers: an observational study
Rev Bras Ter Intensiva. 2014;26(3):269-276
DOI 10.5935/0103-507X.20140038
Views0See moreObjective:
Peripheral perfusion abnormalities are relevant manifestations of shock. Capillary refill time is commonly used for their evaluation. However, the reproducibility of capillary refill time measurements and their correlation with other variables of peripheral perfusion, have not been comprehensively evaluated. Our goal was to determine, in healthy volunteers, the agreement between different methods of capillary refill time quantification and different observers, as well as their correlation with other markers of peripheral perfusion.
Methods:
We studied 63 healthy volunteers. Two observers measured capillary refill time by means of two methods, direct view (CRTchronometer) and video analysis (CRTvideo). We also measured perfusion index (PI) derived from pulse plethysmography and finger pad temperature (Tºperipheral). The agreement between observers and methods was assessed using the Bland and Altman method. Correlations were calculated using Pearson’s correlation. A p-value<0.05 was considered significant.
Results:
The 95% limits of agreement between the two observers were 1.9 sec for CRTchronometer and 1.7 sec for CRTvideo. The 95% limits of agreement between CRTchronometer and CRTvideo were 1.7 sec for observer 1 and 2.3 sec for observer 2. Measurements of CRTchronometer performed by the two observers were correlated with Tºperipheral. Measurements of CRTvideo performed by the two observers were correlated with Tºperipheral and perfusion index.
Conclusion:
In healthy volunteers, measurements of capillary refill time performed by either different observers or different methods showed poor agreement. Nevertheless, capillary refill time still reflected peripheral perfusion as shown by its correlation with objective variables of peripheral perfusion.
-
Original Articles
Urinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
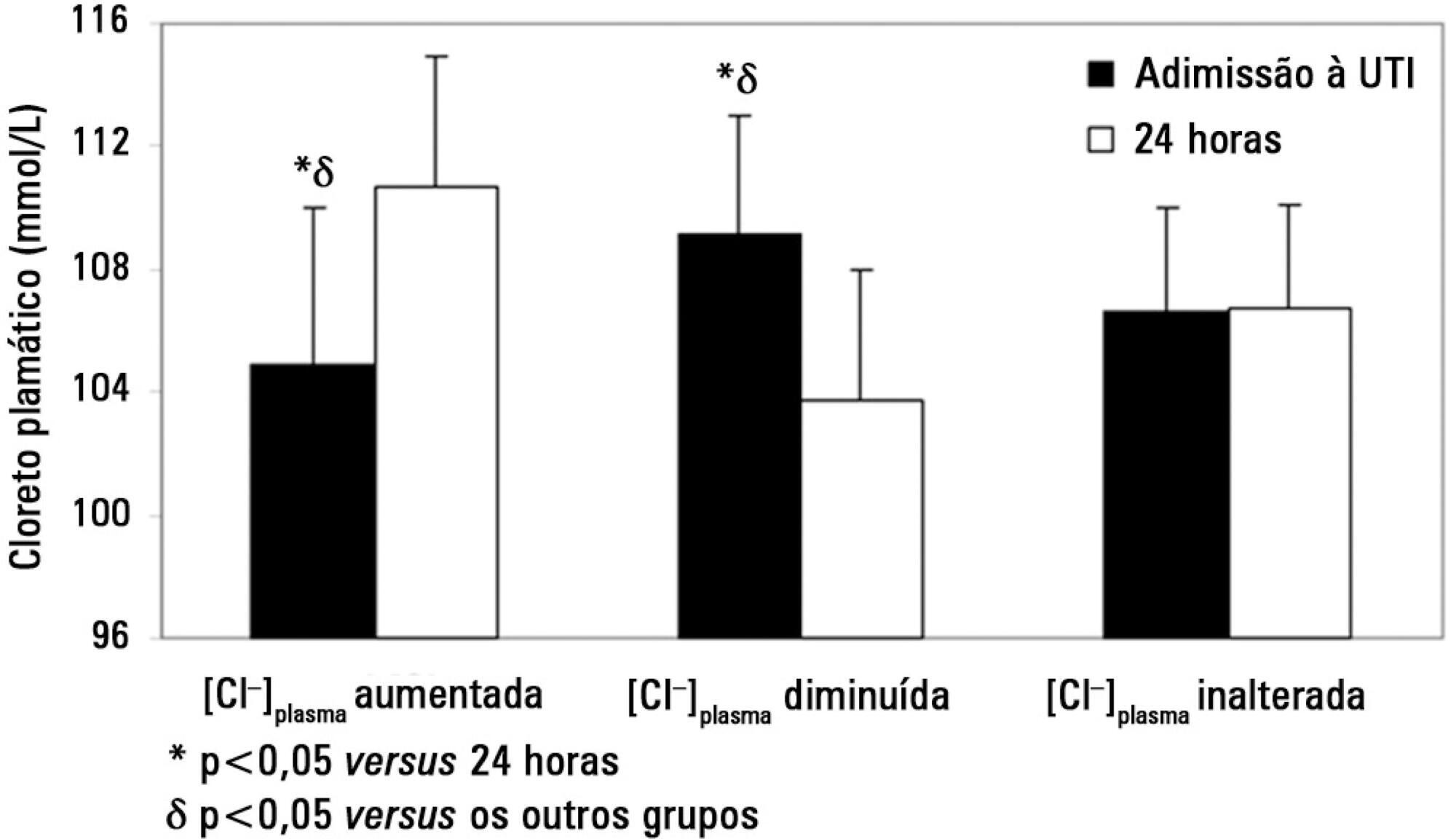
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Views1Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
-
Microcirculation in the intensive care unit
Rev Bras Ter Intensiva. 2011;23(3):249-251
-
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
Views0Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis