Triage Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):38-47
DOI 10.5935/0103-507X.20210004
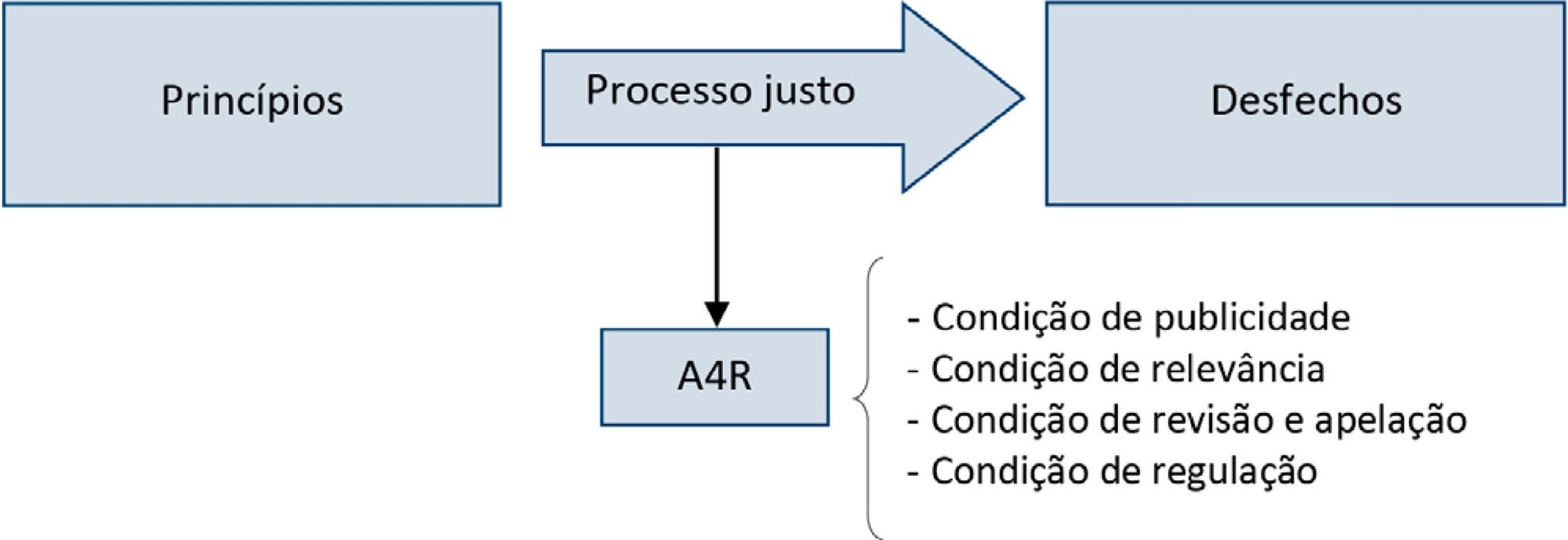
Triage for intensive care unit admission is a frequent event and is associated to worse clinical outcomes. The process of triage is variable and may be influenced by biases and prejudices, which could lead to potentially unfair decisions. The Brazilian Federal Council of Medicine (Conselho Federal de Medicina) has recently released a guideline for intensive care unit admission and discharge. The aim of this paper is to evaluate the ethical dilemmas related to the implementation of this guideline, through the accountability for reasonabless approach, known as A4R, as elaborated by Norman Daniels. We conclude that the guideline contemplates A4R conditions, but we observe that there is a need for indication of A4R-concordant criteria to operationalize the guidelines.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):38-47
DOI 10.5935/0103-507X.20210004
Triage for intensive care unit admission is a frequent event and is associated to worse clinical outcomes. The process of triage is variable and may be influenced by biases and prejudices, which could lead to potentially unfair decisions. The Brazilian Federal Council of Medicine (Conselho Federal de Medicina) has recently released a guideline for intensive care unit admission and discharge. The aim of this paper is to evaluate the ethical dilemmas related to the implementation of this guideline, through the accountability for reasonabless approach, known as A4R, as elaborated by Norman Daniels. We conclude that the guideline contemplates A4R conditions, but we observe that there is a need for indication of A4R-concordant criteria to operationalize the guidelines.