Coronavirus infections Archives - Page 2 of 4 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 - 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 - 55.6 p = 0.02).
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 - 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 - 55.6 p = 0.02).
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):348-353
DOI 10.5935/0103-507X.20200062
A novel coronavirus emerged this year as a cause of viral pneumonia. The main characteristics of the virus are rapid transmission, high contagion capacity and potential severity. The objective of this case series study is to describe the clinical characteristics of patients with confirmed coronavirus disease (COVID-19) admitted to different intensive care units in Argentina for mechanical ventilation.
A descriptive, prospective, multicenter case series study was conducted between April 1 and May 8, 2020. Data from patients older than 18 years who were admitted to the intensive care unit for mechanical ventilation for acute respiratory failure with a positive diagnosis of COVID-19 were included.
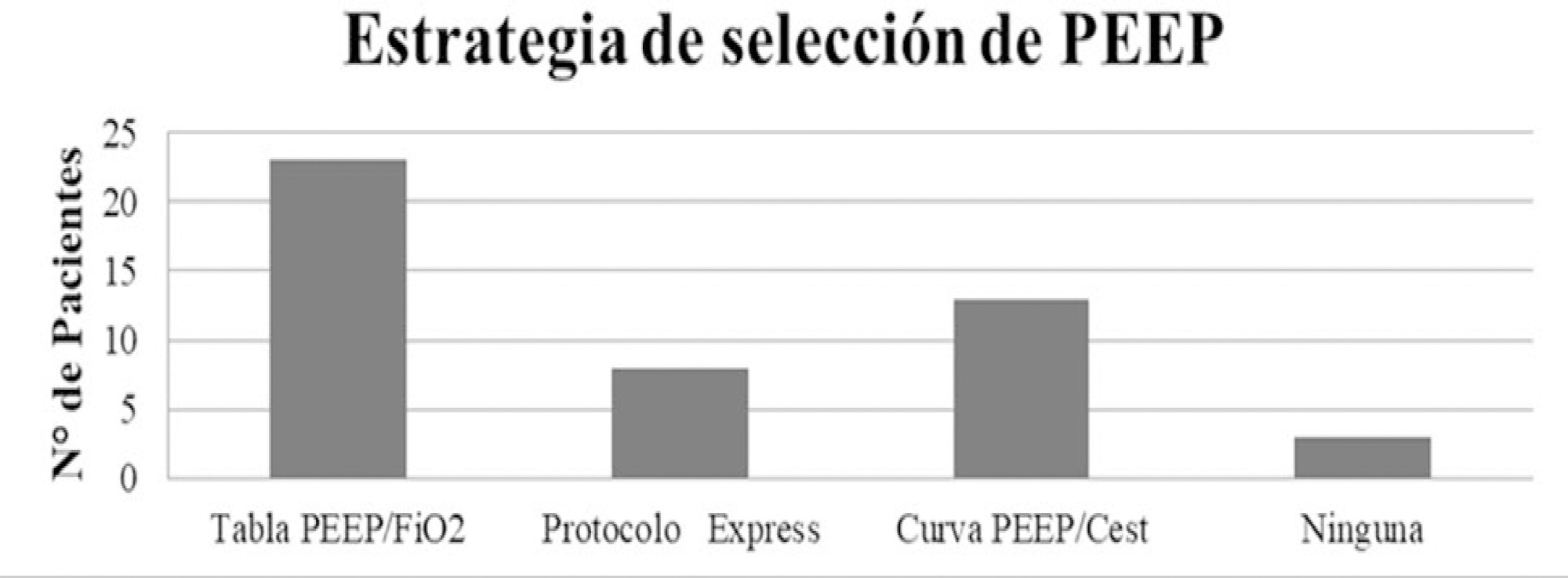
The variables for 47 patients from 31 intensive care units were recorded: 78.7% were men (median age of 61 years), with a SAPS II score of 43 and a Charlson index score of 3. The initial ventilatory mode was volume control - continuous mandatory ventilation with a tidal volume less than 8mL/kg in 100% of cases, with a median positive end-expiratory pressure of 10.5cmH2O. At the end of the study, 29 patients died, 8 were discharged, and 10 remained hospitalized. The SAPS II score was higher among patients who died (p = 0.046). Charlson comorbidity index was associated with higher mortality (OR = 2.27, 95% CI 1.13 - 4.55, p = 0.02).
Patients with COVID-19 and on mechanical ventilation in this series presented clinical variables similar to those described to date in other international reports. Our findings provide data that may predict outcomes.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):348-353
DOI 10.5935/0103-507X.20200062
A novel coronavirus emerged this year as a cause of viral pneumonia. The main characteristics of the virus are rapid transmission, high contagion capacity and potential severity. The objective of this case series study is to describe the clinical characteristics of patients with confirmed coronavirus disease (COVID-19) admitted to different intensive care units in Argentina for mechanical ventilation.
A descriptive, prospective, multicenter case series study was conducted between April 1 and May 8, 2020. Data from patients older than 18 years who were admitted to the intensive care unit for mechanical ventilation for acute respiratory failure with a positive diagnosis of COVID-19 were included.
The variables for 47 patients from 31 intensive care units were recorded: 78.7% were men (median age of 61 years), with a SAPS II score of 43 and a Charlson index score of 3. The initial ventilatory mode was volume control - continuous mandatory ventilation with a tidal volume less than 8mL/kg in 100% of cases, with a median positive end-expiratory pressure of 10.5cmH2O. At the end of the study, 29 patients died, 8 were discharged, and 10 remained hospitalized. The SAPS II score was higher among patients who died (p = 0.046). Charlson comorbidity index was associated with higher mortality (OR = 2.27, 95% CI 1.13 - 4.55, p = 0.02).
Patients with COVID-19 and on mechanical ventilation in this series presented clinical variables similar to those described to date in other international reports. Our findings provide data that may predict outcomes.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):224-228
DOI 10.5935/0103-507X.20200030
To estimate the reporting rates of coronavirus disease 2019 (COVID-19) cases for Brazil as a whole and states.
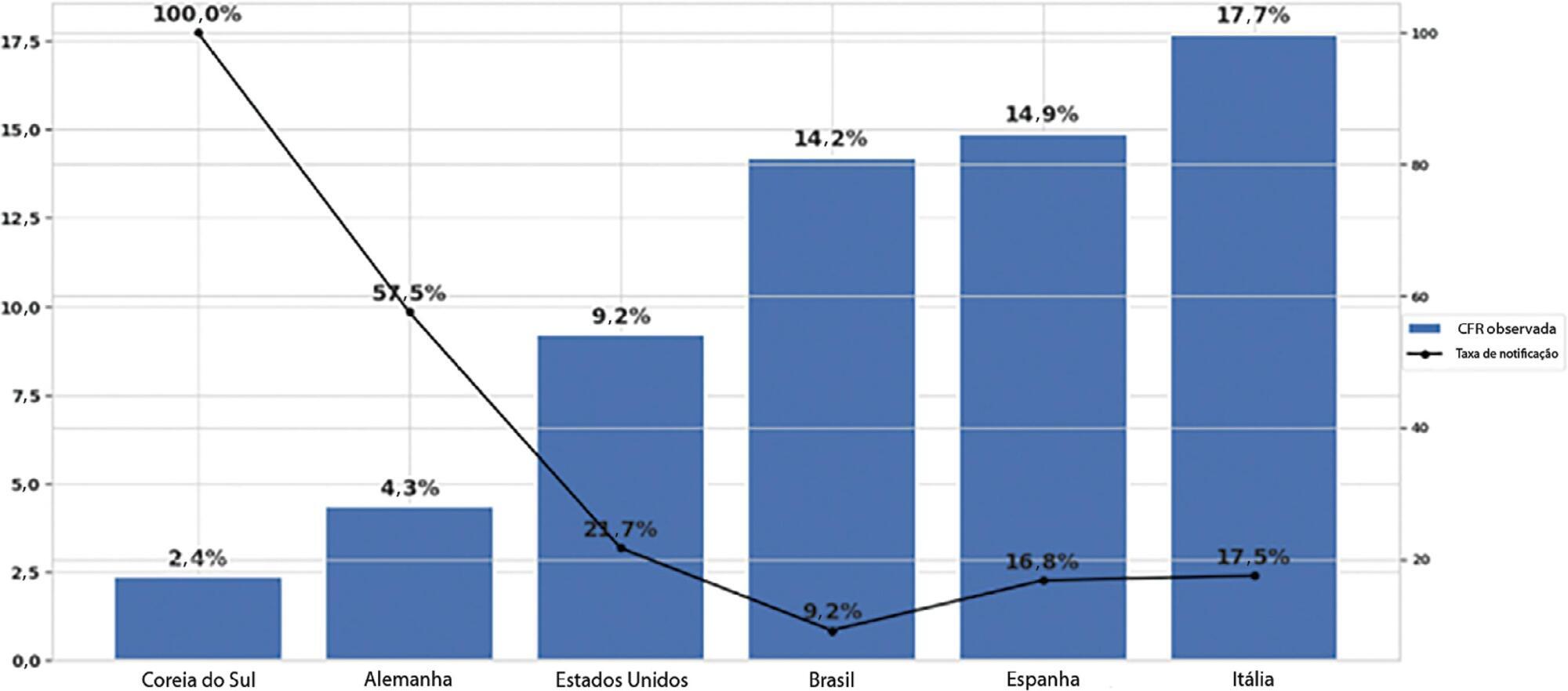
We estimated the actual number of COVID-19 cases using the reported number of deaths in Brazil and each state, and the expected case-fatality ratio from the World Health Organization. Brazil’s expected case-fatality ratio was also adjusted by the population’s age pyramid. Therefore, the notification rate can be defined as the number of confirmed cases (notified by the Ministry of Health) divided by the number of expected cases (estimated from the number of deaths).
The reporting rate for COVID-19 in Brazil was estimated at 9.2% (95%CI 8.8% - 9.5%), with all the states presenting rates below 30%. São Paulo and Rio de Janeiro, the most populated states in Brazil, showed small reporting rates (8.9% and 7.2%, respectively). The highest reporting rate occurred in Roraima (31.7%) and the lowest in Paraiba (3.4%).
The results indicated that the reporting of confirmed cases in Brazil is much lower as compared to other countries we analyzed. Therefore, decision-makers, including the government, fail to know the actual dimension of the pandemic, which may interfere with the determination of control measures.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):224-228
DOI 10.5935/0103-507X.20200030
To estimate the reporting rates of coronavirus disease 2019 (COVID-19) cases for Brazil as a whole and states.
We estimated the actual number of COVID-19 cases using the reported number of deaths in Brazil and each state, and the expected case-fatality ratio from the World Health Organization. Brazil’s expected case-fatality ratio was also adjusted by the population’s age pyramid. Therefore, the notification rate can be defined as the number of confirmed cases (notified by the Ministry of Health) divided by the number of expected cases (estimated from the number of deaths).
The reporting rate for COVID-19 in Brazil was estimated at 9.2% (95%CI 8.8% - 9.5%), with all the states presenting rates below 30%. São Paulo and Rio de Janeiro, the most populated states in Brazil, showed small reporting rates (8.9% and 7.2%, respectively). The highest reporting rate occurred in Roraima (31.7%) and the lowest in Paraiba (3.4%).
The results indicated that the reporting of confirmed cases in Brazil is much lower as compared to other countries we analyzed. Therefore, decision-makers, including the government, fail to know the actual dimension of the pandemic, which may interfere with the determination of control measures.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
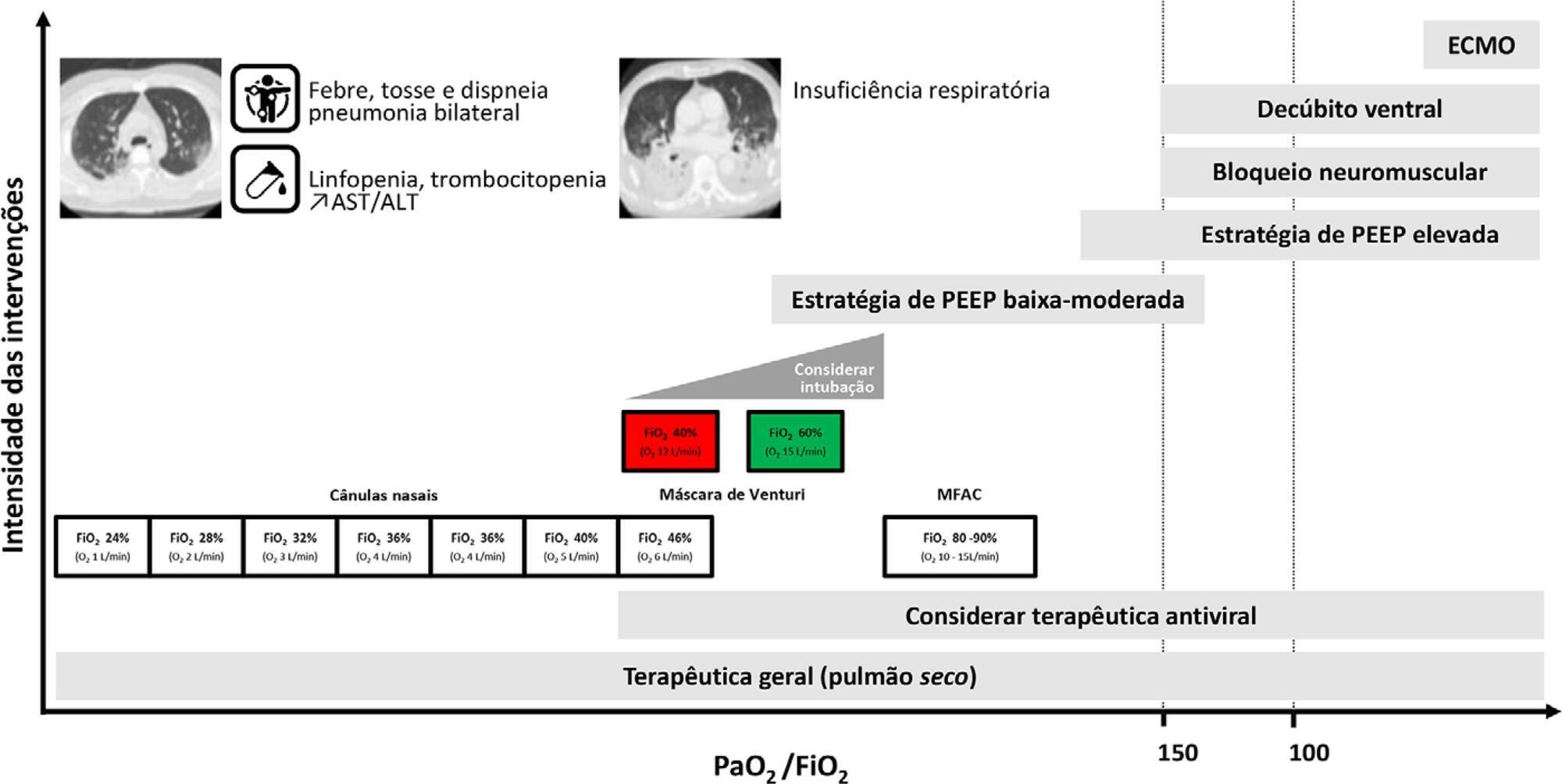
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.