Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Leandro Costa Miranda"
We found (2) results for your search.Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
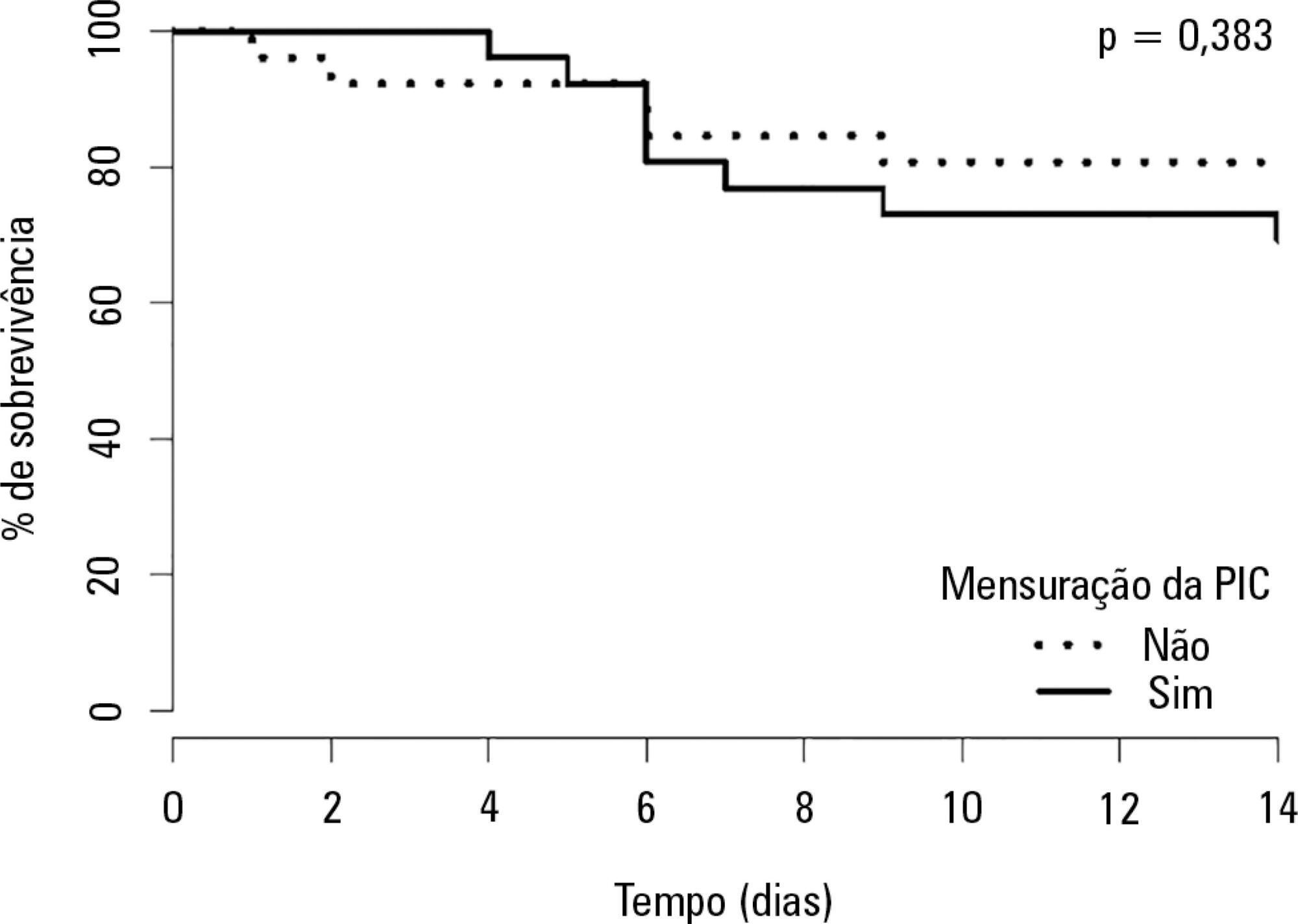
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):421-429
DOI 10.5935/0103-507X.20140065
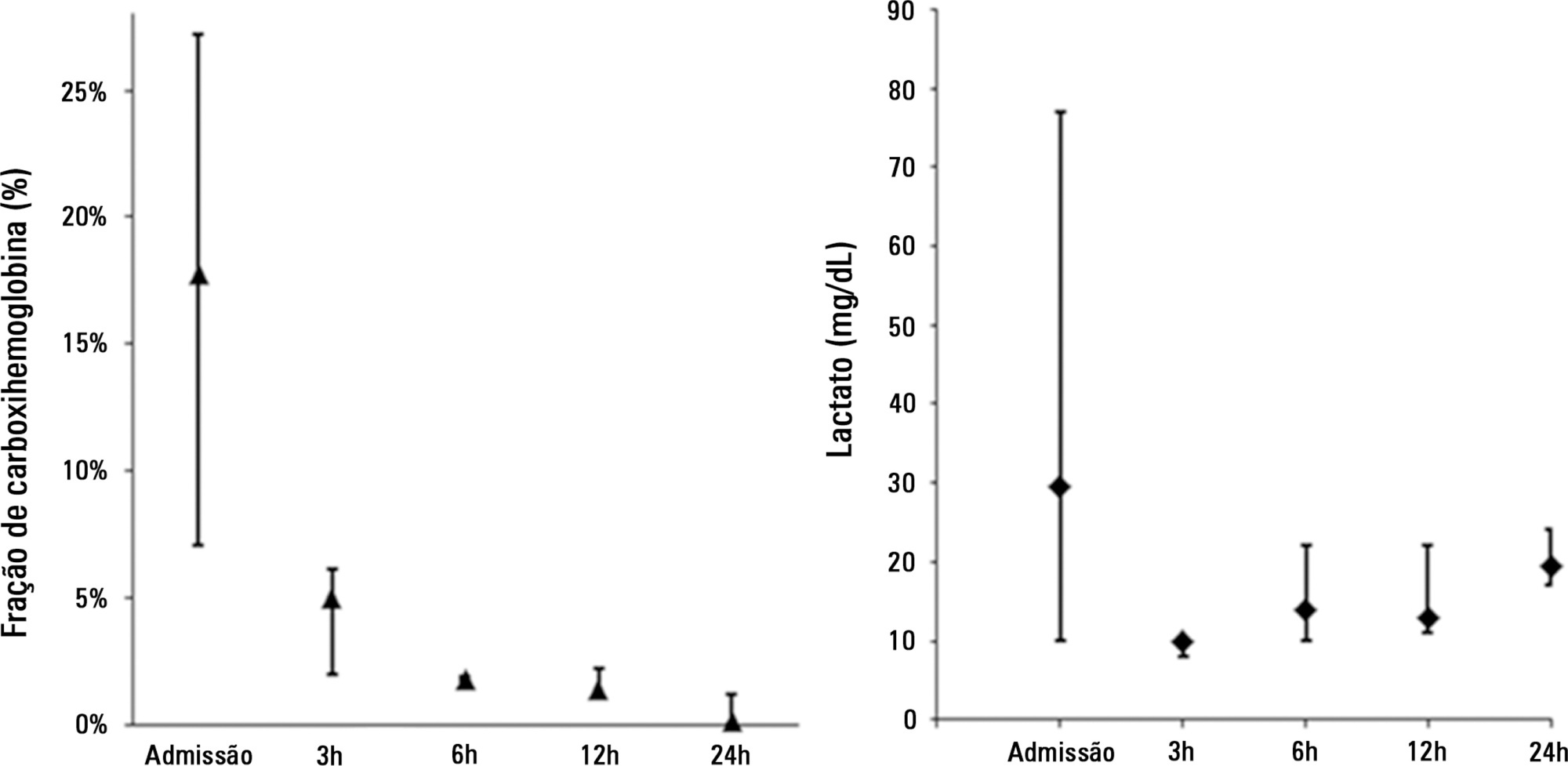
On January 2013, a disaster at Santa Maria (RS) due to a fire in a confined space caused 242 deaths, most of them by inhalation injury. On November 2013, four individuals required intensive care following smoke inhalation from a fire at the Memorial da América Latina in São Paulo (SP). The present article reports the clinical progression and management of disaster victims presenting with inhalation injury. Patients ERL and OC exhibited early respiratory failure, bronchial aspiration of carbonaceous material, and carbon monoxide poisoning. Ventilation support was performed with 100% oxygen, the aspirated material was removed by bronchoscopy, and cyanide poisoning was empirically treated with sodium nitrite and sodium thiosulfate. Patient RP initially exhibited cough and retrosternal burning and subsequently progressed to respiratory failure due to upper airway swelling and early-onset pulmonary infection, which were treated with protective ventilation and antimicrobial agents. This patient was extubated following improvement of edema on bronchoscopy. Patient MA, an asthmatic, exhibited carbon monoxide poisoning and bronchospasm and was treated with normobaric hyperoxia, bronchodilators, and corticosteroids. The length of stay in the intensive care unit varied from four to 10 days, and all four patients exhibited satisfactory functional recovery. To conclude, inhalation injury has a preponderant role in fires in confined spaces. Invasive ventilation should not be delayed in cases with significant airway swelling. Hyperoxia should be induced early as a therapeutic means against carbon monoxide poisoning, in addition to empiric pharmacological treatment in suspected cases of cyanide poisoning.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):421-429
DOI 10.5935/0103-507X.20140065
On January 2013, a disaster at Santa Maria (RS) due to a fire in a confined space caused 242 deaths, most of them by inhalation injury. On November 2013, four individuals required intensive care following smoke inhalation from a fire at the Memorial da América Latina in São Paulo (SP). The present article reports the clinical progression and management of disaster victims presenting with inhalation injury. Patients ERL and OC exhibited early respiratory failure, bronchial aspiration of carbonaceous material, and carbon monoxide poisoning. Ventilation support was performed with 100% oxygen, the aspirated material was removed by bronchoscopy, and cyanide poisoning was empirically treated with sodium nitrite and sodium thiosulfate. Patient RP initially exhibited cough and retrosternal burning and subsequently progressed to respiratory failure due to upper airway swelling and early-onset pulmonary infection, which were treated with protective ventilation and antimicrobial agents. This patient was extubated following improvement of edema on bronchoscopy. Patient MA, an asthmatic, exhibited carbon monoxide poisoning and bronchospasm and was treated with normobaric hyperoxia, bronchodilators, and corticosteroids. The length of stay in the intensive care unit varied from four to 10 days, and all four patients exhibited satisfactory functional recovery. To conclude, inhalation injury has a preponderant role in fires in confined spaces. Invasive ventilation should not be delayed in cases with significant airway swelling. Hyperoxia should be induced early as a therapeutic means against carbon monoxide poisoning, in addition to empiric pharmacological treatment in suspected cases of cyanide poisoning.