Trauma severity indices Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(4):397-406
DOI 10.5935/0103-507X.20140061
Severe trauma can be associated with significant hemorrhagic shock and impaired organ perfusion. We hypothesized that goal-directed therapy would confer morbidity and mortality benefits in major trauma.
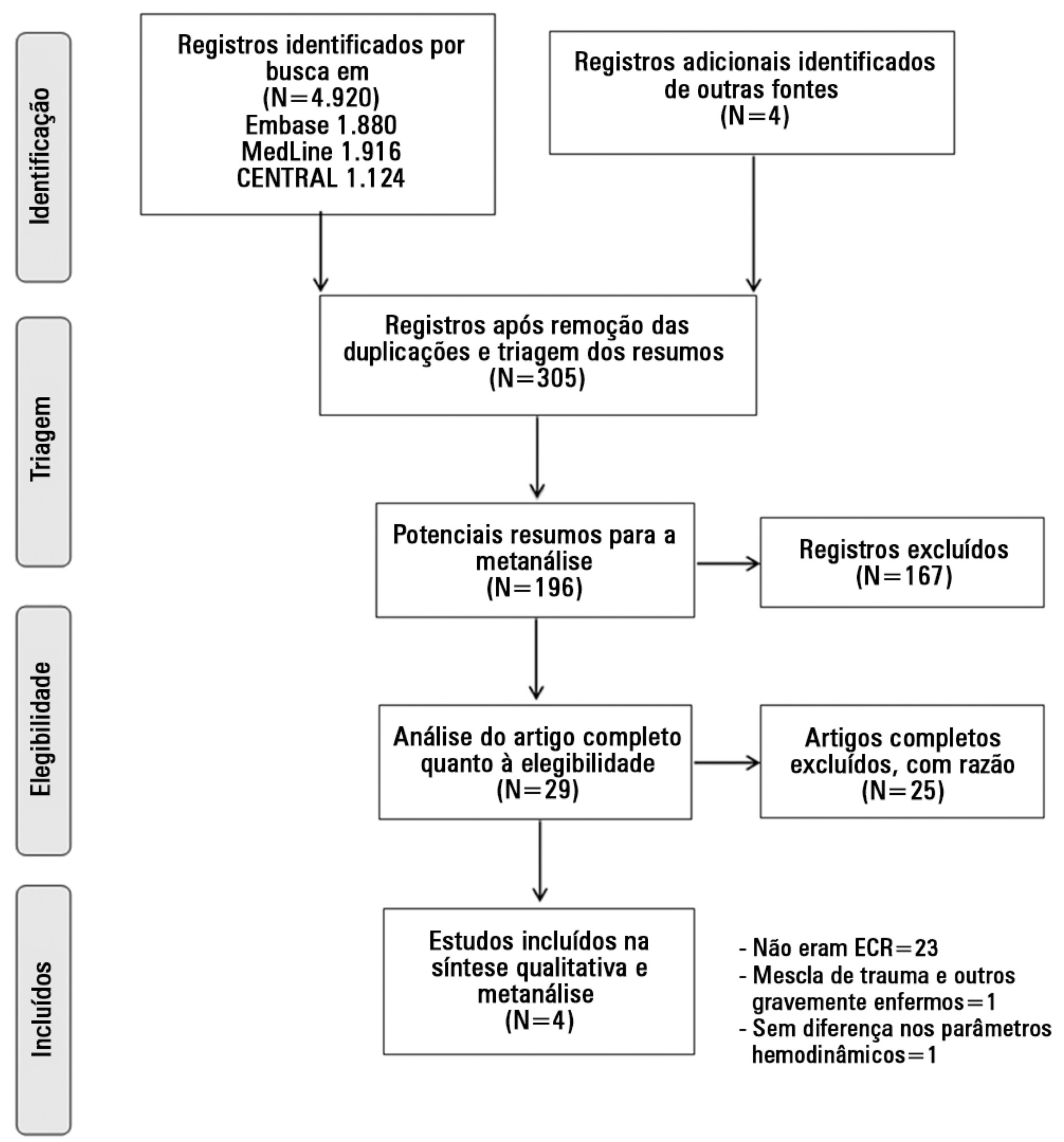
The MedLine, Embase and Cochrane Controlled Clinical Trials Register databases were systematically searched for randomized, controlled trials of goal-directed therapy in severe trauma patients. Mortality was the primary outcome of this review. Secondary outcomes included complication rates, length of hospital and intensive care unit stay, and the volume of fluid and blood administered. Meta-analysis was performed using RevMan software, and the data presented are as odds ratios for dichotomous outcomes and as mean differences (MDs) and standard MDs for continuous outcomes.
Four randomized, controlled trials including 419 patients were analyzed. Mortality risk was significantly reduced in goal-directed therapy-treated patients, compared to the control group (OR=0.56, 95%CI: 0.34-0.92). Intensive care (MD: 3.7 days 95%CI: 1.06-6.5) and hospital length of stay (MD: 3.5 days, 95%CI: 2.75-4.25) were significantly shorter in the protocol group patients. There were no differences in reported total fluid volume or blood transfusions administered. Heterogeneity in reporting among the studies prevented quantitative analysis of complications.
Following severe trauma, early goal-directed therapy was associated with lower mortality and shorter durations of intensive care unit and hospital stays. The findings of this analysis should be interpreted with caution due to the presence of significant heterogeneity and the small number of the randomized, controlled trials included.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):397-406
DOI 10.5935/0103-507X.20140061
Severe trauma can be associated with significant hemorrhagic shock and impaired organ perfusion. We hypothesized that goal-directed therapy would confer morbidity and mortality benefits in major trauma.
The MedLine, Embase and Cochrane Controlled Clinical Trials Register databases were systematically searched for randomized, controlled trials of goal-directed therapy in severe trauma patients. Mortality was the primary outcome of this review. Secondary outcomes included complication rates, length of hospital and intensive care unit stay, and the volume of fluid and blood administered. Meta-analysis was performed using RevMan software, and the data presented are as odds ratios for dichotomous outcomes and as mean differences (MDs) and standard MDs for continuous outcomes.
Four randomized, controlled trials including 419 patients were analyzed. Mortality risk was significantly reduced in goal-directed therapy-treated patients, compared to the control group (OR=0.56, 95%CI: 0.34-0.92). Intensive care (MD: 3.7 days 95%CI: 1.06-6.5) and hospital length of stay (MD: 3.5 days, 95%CI: 2.75-4.25) were significantly shorter in the protocol group patients. There were no differences in reported total fluid volume or blood transfusions administered. Heterogeneity in reporting among the studies prevented quantitative analysis of complications.
Following severe trauma, early goal-directed therapy was associated with lower mortality and shorter durations of intensive care unit and hospital stays. The findings of this analysis should be interpreted with caution due to the presence of significant heterogeneity and the small number of the randomized, controlled trials included.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):220-228
DOI 10.1590/S0103-507X2010000300002
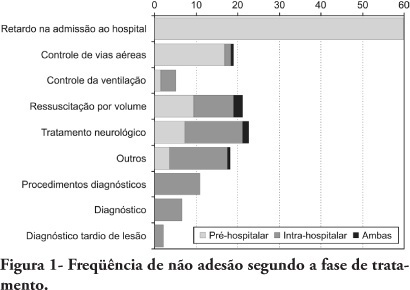
OBJECTIVES: To evaluate patients treated for traumatic injuries and to identify adherence to guidelines recommendations of treatment and association with death. The recommendations adopted were defined by the committee on trauma of the American College of Surgeons in advanced trauma life support. METHODS: Retrospective cohort study conducted at a teaching hospital. The study population was victims of trauma > 12 years of age with injury severity scores > 16 who were treated between January 1997 and December 2001. Data collection was divided into three phases: pre-hospital, in-hospital, and post-mortem. The data collected were analyzed using EPI INFO. RESULTS: We analyzed 207 patients, 147 blunt trauma victims (71%) and 60 (29%) penetrating trauma victims. Trauma victims had a 40.1% mortality rate. We identified 221 non adherence events that occurred in 137 patients. We found a mean of 1.61 non adherence per patient, and it occurred less frequently in survivors (1.4) than in non-survivors (1.9; p=0.033). According to the trauma score and injury severity score methodology, 54.2% of deaths were considered potentially preventable. Non adherence occurred 1.77 times more frequently in those considered potentially preventable deaths compared to other non-survivors (95% CI: 1.12-2.77; p=0.012), and 92.9% of the multiple non adherence occurred in the first group (p=0.029). CONCLUSIONS: Non adherence occurred more frequently in patients with potentially preventable deaths. Non adherence to guidelines recommendations can be considered a contributing factor to death in trauma victims and can lead to an increase in the number of potentially preventable deaths.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):220-228
DOI 10.1590/S0103-507X2010000300002
OBJECTIVES: To evaluate patients treated for traumatic injuries and to identify adherence to guidelines recommendations of treatment and association with death. The recommendations adopted were defined by the committee on trauma of the American College of Surgeons in advanced trauma life support. METHODS: Retrospective cohort study conducted at a teaching hospital. The study population was victims of trauma > 12 years of age with injury severity scores > 16 who were treated between January 1997 and December 2001. Data collection was divided into three phases: pre-hospital, in-hospital, and post-mortem. The data collected were analyzed using EPI INFO. RESULTS: We analyzed 207 patients, 147 blunt trauma victims (71%) and 60 (29%) penetrating trauma victims. Trauma victims had a 40.1% mortality rate. We identified 221 non adherence events that occurred in 137 patients. We found a mean of 1.61 non adherence per patient, and it occurred less frequently in survivors (1.4) than in non-survivors (1.9; p=0.033). According to the trauma score and injury severity score methodology, 54.2% of deaths were considered potentially preventable. Non adherence occurred 1.77 times more frequently in those considered potentially preventable deaths compared to other non-survivors (95% CI: 1.12-2.77; p=0.012), and 92.9% of the multiple non adherence occurred in the first group (p=0.029). CONCLUSIONS: Non adherence occurred more frequently in patients with potentially preventable deaths. Non adherence to guidelines recommendations can be considered a contributing factor to death in trauma victims and can lead to an increase in the number of potentially preventable deaths.