Urine/analysis Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
To show that alterations in the plasma chloride concentration ([Cl-]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
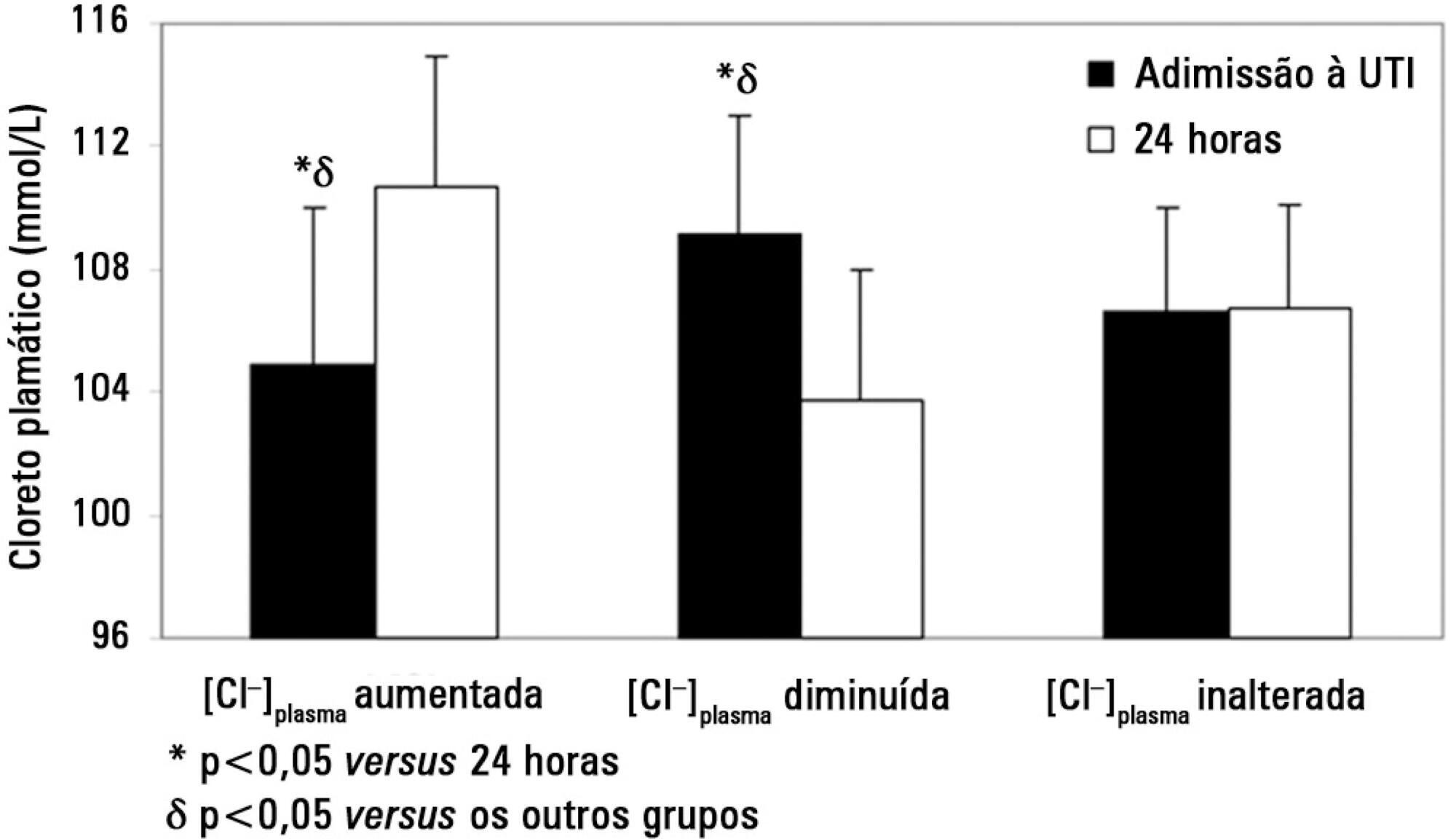
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl-]plasma at the 24 hours time point: increased [Cl-]plasma (n=39), decreased [Cl-]plasma (n=56) or unchanged [Cl-]plasma (n=53).
On admission, the increased [Cl-]plasma group had a lower [Cl-]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl-]plasma group showed a higher [Cl-]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl-]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl-]plasma on admission and [SID]urine were independent predictors of the variation in [Cl-]plasma 24 hours later.
Changes in [Cl-]plasma during the first postoperative day were largely related to [SID]urine and [Cl-]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
To show that alterations in the plasma chloride concentration ([Cl-]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl-]plasma at the 24 hours time point: increased [Cl-]plasma (n=39), decreased [Cl-]plasma (n=56) or unchanged [Cl-]plasma (n=53).
On admission, the increased [Cl-]plasma group had a lower [Cl-]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl-]plasma group showed a higher [Cl-]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl-]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl-]plasma on admission and [SID]urine were independent predictors of the variation in [Cl-]plasma 24 hours later.
Changes in [Cl-]plasma during the first postoperative day were largely related to [SID]urine and [Cl-]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.