Acid-base equilibrium Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
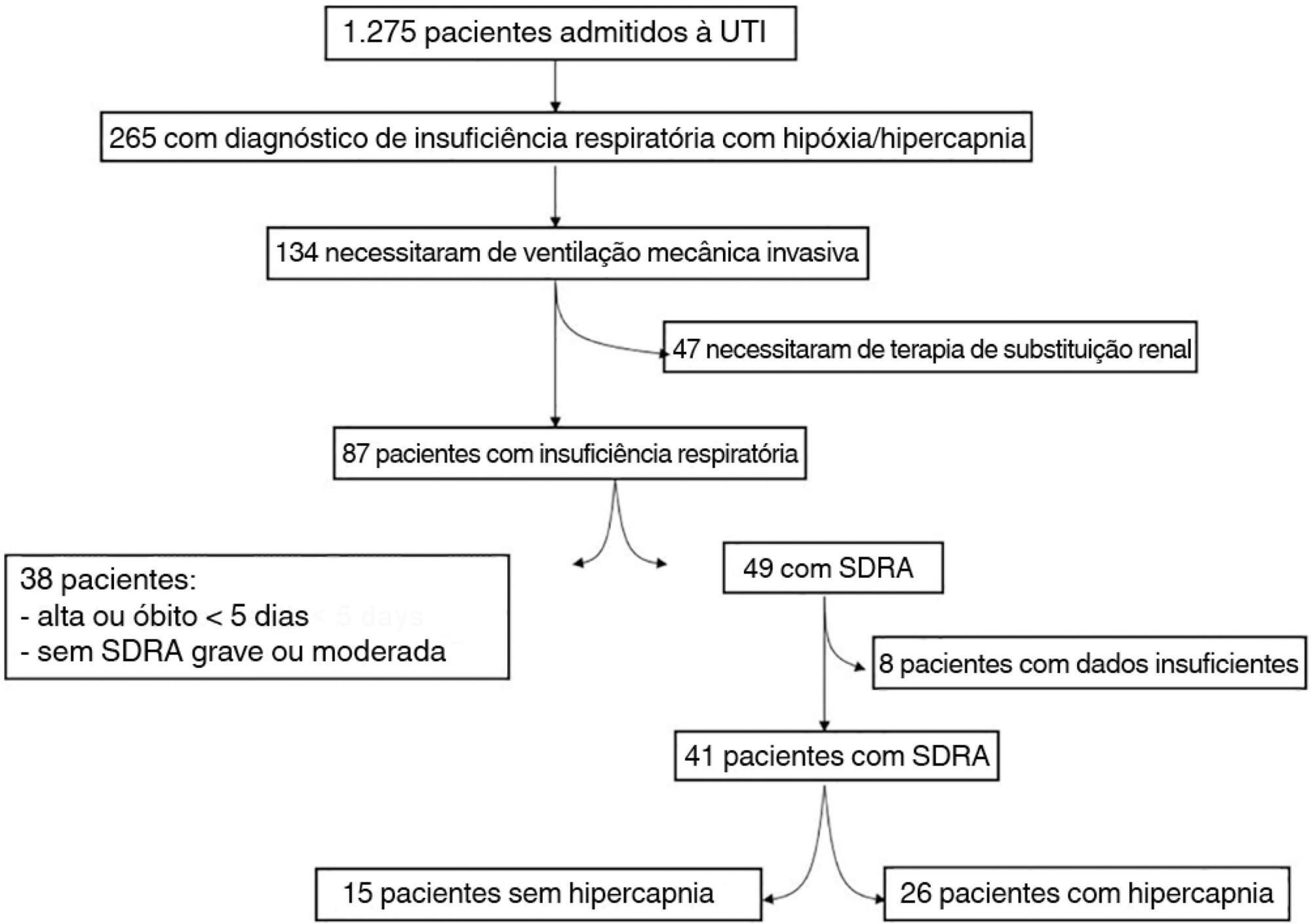
The data were retrieved from a prospective collected database. Variables from patients' admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
The data were retrieved from a prospective collected database. Variables from patients' admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):176-182
DOI 10.1590/S0103-507X2011000200010
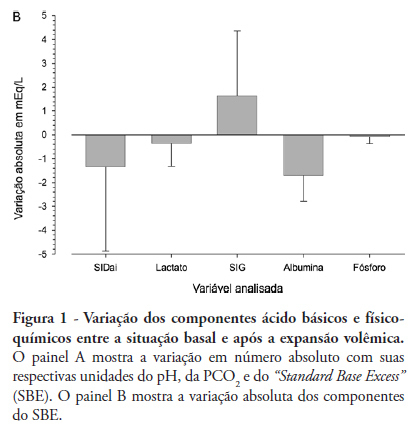
OBJECTIVE: The aim of this study was to characterize and quantify metabolic acidosis that was caused by initial volume expansion during the reanimation of patients with severe sepsis and septic shock. METHODS: A blood sample was drawn for physicochemical characterization of the patient's acid-base equilibrium both before and after volume expansion using 30 mL/kg 0.9% saline solution. The diagnosis and quantification of metabolic acidosis were based on the standard base excess (SBE). RESULTS: Eight patients with a mean age of 58 ± 13 years and mean APACHE II scores of 20 ± 4 were expanded using 2,000 ± 370 mL of 0.9% saline solution. Blood pH dropped from 7.404 ± 0.080 to 7.367 ± 0.086 (p=0.018), and PC O2 increased from 30 ± 5 to 32 ± 2 mmHg (p=0.215); SBE dropped from -4.4 ± 5.6 to -6.0 ± 5.7 mEq/L (p=0.039). The drop in SBE was associated with the acidifying power of two factors, namely, a significant increase in the strong ion gap (SIG) from 6.1 ± 3.4 to 7.7 ± 4.0 mEq/L (p = 0.134) and a non-significant drop in the apparent inorganic strong ion differences (SIDai) from 40 ± 5 to 38 ± 4 mEq/L (p = 0.318). Conversely, the serum albumin levels decreased from 3.1 ± 1.0 to 2.6 ± 0.8 mEq/L (p = 0.003) with an alkalinizing effect on SBE. Increased serum chloride levels from 103 ± 10 to 106 ± 7 mEq/L (p < 0.001) led to a drop in SIDai. CONCLUSION: Initial resuscitation using 30 mL/kg of 0.9% saline solution for patients with severe sepsis and septic shock is associated with worsened metabolic acidosis, as measured by SBE. This worsened SBE can be ascribed to a serum increase in the levels of unmeasurable anions and chloride.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):176-182
DOI 10.1590/S0103-507X2011000200010
OBJECTIVE: The aim of this study was to characterize and quantify metabolic acidosis that was caused by initial volume expansion during the reanimation of patients with severe sepsis and septic shock. METHODS: A blood sample was drawn for physicochemical characterization of the patient's acid-base equilibrium both before and after volume expansion using 30 mL/kg 0.9% saline solution. The diagnosis and quantification of metabolic acidosis were based on the standard base excess (SBE). RESULTS: Eight patients with a mean age of 58 ± 13 years and mean APACHE II scores of 20 ± 4 were expanded using 2,000 ± 370 mL of 0.9% saline solution. Blood pH dropped from 7.404 ± 0.080 to 7.367 ± 0.086 (p=0.018), and PC O2 increased from 30 ± 5 to 32 ± 2 mmHg (p=0.215); SBE dropped from -4.4 ± 5.6 to -6.0 ± 5.7 mEq/L (p=0.039). The drop in SBE was associated with the acidifying power of two factors, namely, a significant increase in the strong ion gap (SIG) from 6.1 ± 3.4 to 7.7 ± 4.0 mEq/L (p = 0.134) and a non-significant drop in the apparent inorganic strong ion differences (SIDai) from 40 ± 5 to 38 ± 4 mEq/L (p = 0.318). Conversely, the serum albumin levels decreased from 3.1 ± 1.0 to 2.6 ± 0.8 mEq/L (p = 0.003) with an alkalinizing effect on SBE. Increased serum chloride levels from 103 ± 10 to 106 ± 7 mEq/L (p < 0.001) led to a drop in SIDai. CONCLUSION: Initial resuscitation using 30 mL/kg of 0.9% saline solution for patients with severe sepsis and septic shock is associated with worsened metabolic acidosis, as measured by SBE. This worsened SBE can be ascribed to a serum increase in the levels of unmeasurable anions and chloride.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
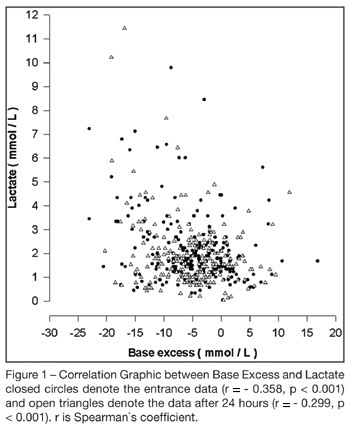
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.