
You searched for:"José Mauro da Fonseca Pestana Ribeiro"
We found (1) results for your search.-
Review Articles
Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons
 ,
, - Rogerio Zigaib, [ … ],
- Marcelo Park
Abstract
Review ArticlesExtracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons ,
- Rogerio Zigaib,
- José Mauro da Fonseca Pestana Ribeiro,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Marcelo Park
Views0ABSTRACT
Objective:
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
Methods:
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Results:
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% – 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 – 0.95 and RR: 0.68; 95%CI 0.55 – 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 – 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th – P75th: 12.49 – 17.18) and P50th 29.80 (P25th – P75th: 26.04 – 33.56] days, respectively.
Conclusion:
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Keywords:Extracorporeal membrane oxygenationIntensive care unitsMeta-analysisRespiratory distress syndrome, adultRespiratory insufficiencySee moreViews0

Abstract
Review ArticlesExtracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons ,
- Rogerio Zigaib,
- José Mauro da Fonseca Pestana Ribeiro,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Marcelo Park
Views0ABSTRACT
Objective:
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
Methods:
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Results:
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% – 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 – 0.95 and RR: 0.68; 95%CI 0.55 – 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 – 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th – P75th: 12.49 – 17.18) and P50th 29.80 (P25th – P75th: 26.04 – 33.56] days, respectively.
Conclusion:
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Keywords:Extracorporeal membrane oxygenationIntensive care unitsMeta-analysisRespiratory distress syndrome, adultRespiratory insufficiencySee more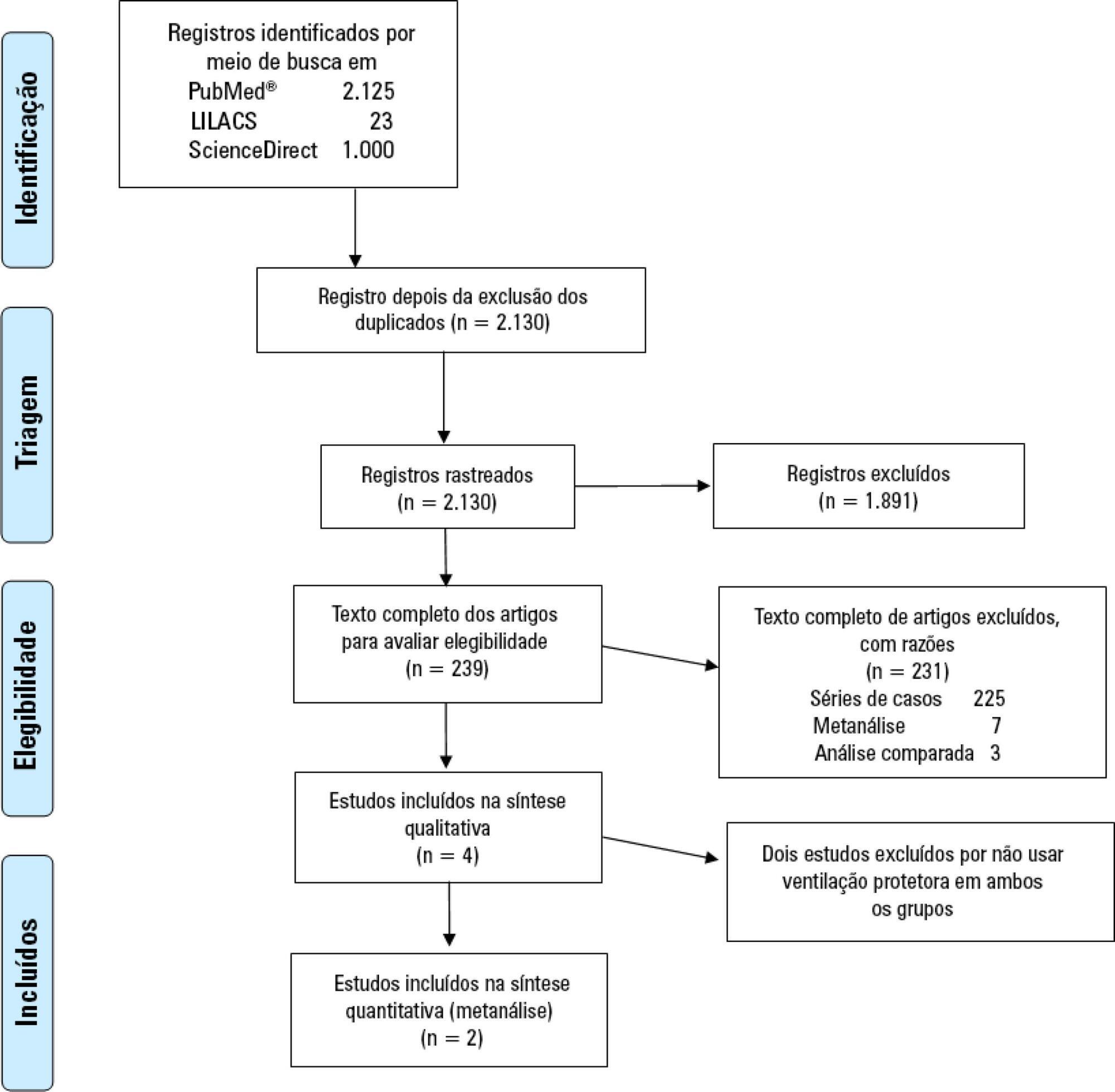
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis