Neurologic manifestations Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(3):412-421
DOI 10.5935/0103-507X.20210065
To calculate mean dilation velocities for Glasgow coma scale-derived injury severity classifications stratified by multiple confounding variables.
In this study, we examined 68,813 pupil readings from 3,595 patients to determine normal dilation velocity with brain injury categorized based upon a Glasgow coma scale as mild (13 - 15), moderate (9 - 12), or severe (3 - 8). The variables age, sex, race, pupil size, intensive care unit length of stay, intracranial pressure, use of narcotics, Glasgow coma scale, and diagnosis were considered as confounding and controlled for in statistical analysis. Machine learning classification algorithm-based logistic regression was employed to identify dilation velocity cutoffs for Glasgow coma scale categories.
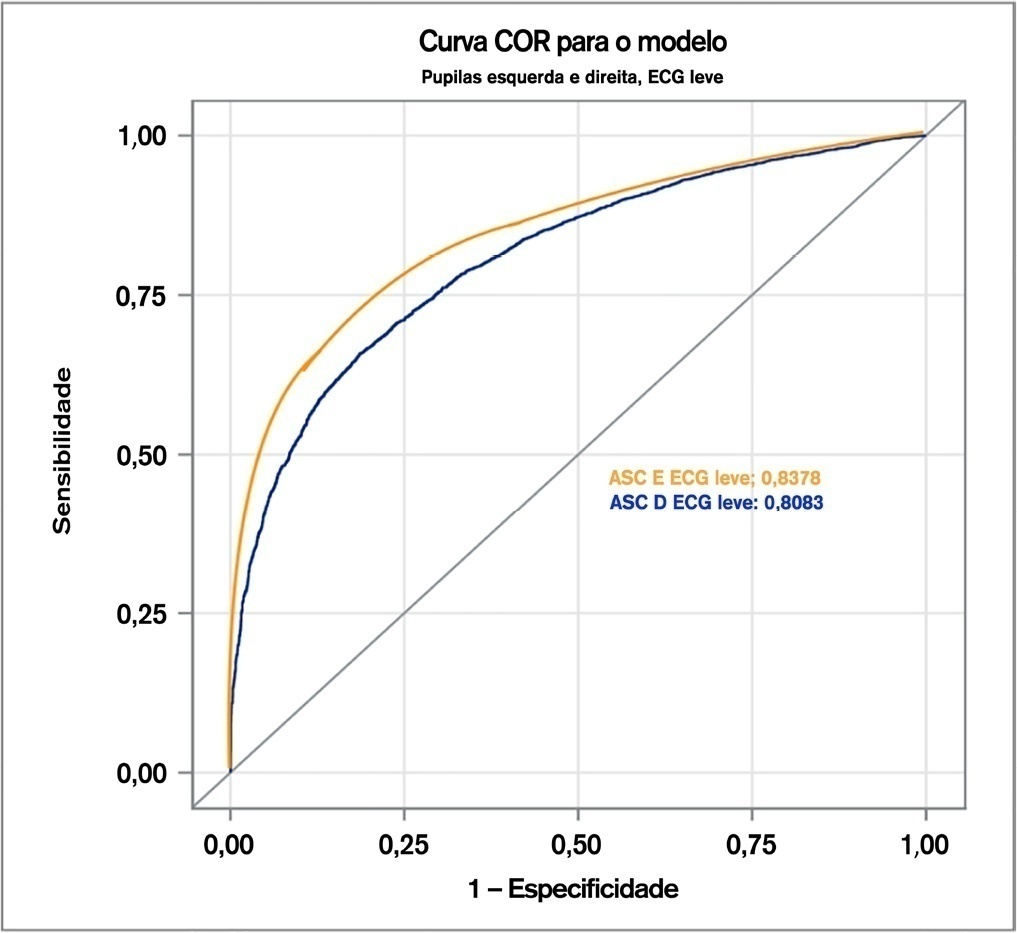
The odds ratios and confidence intervals of these factors were shown to be statistically significant in their influence on dilation velocity. Classification based on the area under the curve showed that for the mild Glasgow coma scale, the dilation velocity threshold value was 1.2mm/s, with false probability rates of 0.1602 and 0.1902 and areas under the curve of 0.8380 and 0.8080 in the left and right eyes, respectively. For the moderate Glasgow coma scale, the dilation velocity was 1.1mm/s, with false probability rates of 0.1880 and 0.1940 and areas under the curve of 0.8120 and 0.8060 in the left and right eyes, respectively. Furthermore, for the severe Glasgow coma scale, the dilation velocity was 0.9mm/s, with false probability rates of 0.1980 and 0.2060 and areas under the curve of 0.8020 and 0.7940 in the left and right eyes, respectively. These values were different from the previous method of subjective description and from previously estimated normal dilation velocities.
Slower dilation velocities were observed in patients with lower Glasgow coma scores, indicating that decreasing velocities may indicate a higher degree of neuronal injury.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):412-421
DOI 10.5935/0103-507X.20210065
To calculate mean dilation velocities for Glasgow coma scale-derived injury severity classifications stratified by multiple confounding variables.
In this study, we examined 68,813 pupil readings from 3,595 patients to determine normal dilation velocity with brain injury categorized based upon a Glasgow coma scale as mild (13 - 15), moderate (9 - 12), or severe (3 - 8). The variables age, sex, race, pupil size, intensive care unit length of stay, intracranial pressure, use of narcotics, Glasgow coma scale, and diagnosis were considered as confounding and controlled for in statistical analysis. Machine learning classification algorithm-based logistic regression was employed to identify dilation velocity cutoffs for Glasgow coma scale categories.
The odds ratios and confidence intervals of these factors were shown to be statistically significant in their influence on dilation velocity. Classification based on the area under the curve showed that for the mild Glasgow coma scale, the dilation velocity threshold value was 1.2mm/s, with false probability rates of 0.1602 and 0.1902 and areas under the curve of 0.8380 and 0.8080 in the left and right eyes, respectively. For the moderate Glasgow coma scale, the dilation velocity was 1.1mm/s, with false probability rates of 0.1880 and 0.1940 and areas under the curve of 0.8120 and 0.8060 in the left and right eyes, respectively. Furthermore, for the severe Glasgow coma scale, the dilation velocity was 0.9mm/s, with false probability rates of 0.1980 and 0.2060 and areas under the curve of 0.8020 and 0.7940 in the left and right eyes, respectively. These values were different from the previous method of subjective description and from previously estimated normal dilation velocities.
Slower dilation velocities were observed in patients with lower Glasgow coma scores, indicating that decreasing velocities may indicate a higher degree of neuronal injury.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):457-460
DOI 10.5935/0103-507X.20210067
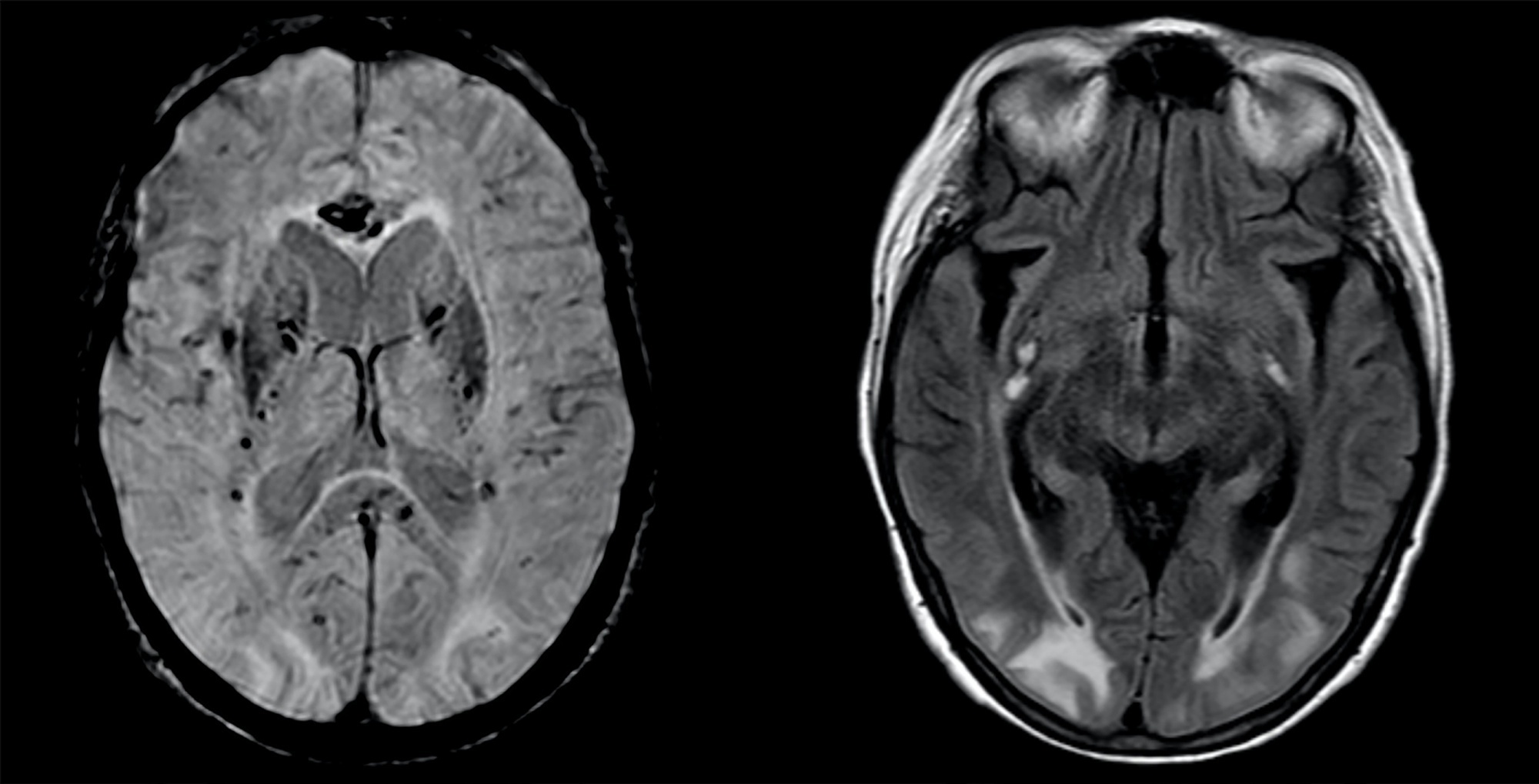
A 63-year-old woman presented to the emergency department with an acute history of fever, prostration and dyspnea. She was diagnosed with severe COVID-19 acute respiratory distress syndrome and, despite optimized critical care support, met the indications for veno-venous extracorporeal membrane oxygenation. On day 34, after 7 days of wean sedation with a positive evolution of neurologic status, she presented a limited generalized tonic-clonic seizure not related to hydroelectrolytic or metabolic imbalance, which led to a diagnostic investigation; her brain imaging tests showed a posterior reversible encephalopathy syndrome. This case emphasizes the issue of neurological complications in patients with severe COVID-19 infection and the importance of early diagnosis and support.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):457-460
DOI 10.5935/0103-507X.20210067
A 63-year-old woman presented to the emergency department with an acute history of fever, prostration and dyspnea. She was diagnosed with severe COVID-19 acute respiratory distress syndrome and, despite optimized critical care support, met the indications for veno-venous extracorporeal membrane oxygenation. On day 34, after 7 days of wean sedation with a positive evolution of neurologic status, she presented a limited generalized tonic-clonic seizure not related to hydroelectrolytic or metabolic imbalance, which led to a diagnostic investigation; her brain imaging tests showed a posterior reversible encephalopathy syndrome. This case emphasizes the issue of neurological complications in patients with severe COVID-19 infection and the importance of early diagnosis and support.